Poster
|
08:00 – 17:00
|
Poster |
|
|
Hauptreferat
|
||
|
P1
La souffrance en soins palliatifs oncologiques : vers une approche intégrative pharmaceutique-spirituelle
Emile Abou Chaar, Fribourg CH
AbstractContexte La souffrance des patients en soins palliatifs oncologiques est souvent décrite comme une douleur totale, concept définie par Cicely Saunders, comme englobant non seulement la dimension physique, mais aussi psychologique, sociale et spirituelle. L’intégration des dimensions spirituelles et/ou religieuses (S/R) dans les soins pourrait améliorer la compréhension de cette souffrance, renforcer les capacités d’adaptation des patients et améliorer leur qualité de vie. Toutefois, cette intégration demeure peu étudiée dans une perspective précoce, notamment dans un contexte de cancer métastatique. Notre projet vise ainsi à mieux comprendre cette souffrance multidimensionnelle et à co-construire une approche personnalisée et intégrative de soulagement précoce. Il explore l’articulation entre l’expérience vécue de la souffrance et les conditions de mise en œuvre d’une approche novatrice, dite pharmaceutique-spirituelle (PHARMA-S-SPIR), combinant soins pharmaceutiques et soins spirituels. Objectiv Explorer comment les patients récemment diagnostiqués avec un cancer métastatique expriment leur souffrance, à qui ils s’adressent, quel rôle jouent les dimensions S/R dans leurs mécanismes d’adaptation, et identifier les défis et les leviers à l’intégration de l’approche PHARMA-S-SPIR dans la pratique clinique. Méthode Conçue avec des patients-partenaires, cette étude adoptera une méthodologie qualitative phénoménologique, basée sur des entrevues semi-dirigées. Environs 30 patients adultes, diagnostiqués depuis moins de 3 mois avec un cancer métastatique, seront recrutés du CHU de Québec-Université Laval (Canada) à l’été 2025. L’analyse thématique des données se fera à l’aide de NVivo. Les thèmes émergents seront ensuite discutés en groupes (focus groups) réunissant de nombreux acteurs du système de santé, y compris soignants et patients-partenaires, afin de réfléchir collectivement aux conditions d’implémentation de cette approche novatrice. Une analyse comparative avec le contexte suisse est également prévue. Résultats Les résultats éclaireront la façon dont la souffrance est perçue, exprimée et prise en charge. Ils mettront en lumière les dynamiques entre les différentes dimensions de la douleur, les stratégies d’adaptation mobilisées et la réceptivité envers l’approche PHARMA-S-SPIR. Conclusion Ce projet vise à repenser la réponse à la souffrance en soins palliatifs en mobilisant une « communauté de soins » interdisciplinaire, engagée dans une prise en charge précoce, globale et centrée sur la personne. |
||
|
P2
Innovation pédagogique dans l’enseignement des soins palliatifs en formation prégraduée
Raffaella D’orio, Blonay CH
Abstract
Contexte
La formation en soins palliatifs constitue un élément essentiel de la formation initiale des professionnels de santé afin de garantir une prise en charge optimale. Toutefois, la transition entre les connaissances théoriques et la pratique clinique représente un défi majeur pour les étudiants en médecine et en soins infirmiers. Plusieurs programmes académiques ont recours à des expériences d’immersion clinique pour réduire cet écart. Dans cette optique, nous avons développé une formation immersive au sein d’une unité spécialisée en soins palliatifs, visant à offrir une expérience d’apprentissage unique. Objectiv Offrir aux étudiants une opportunité d’apprentissage clinique afin de renforcer leurs compétences pratiques en soins palliatifs et de favoriser la collaboration interprofessionnelle. Méthode Ce programme pédagogique innovant s’inscrit dans une formation interprofessionnelle destinée aux étudiants en médecine et en soins infirmiers. Il combine plusieurs méthodes d’enseignement animées par des experts en soins palliatifs : séminaires, simulations, études de cas, travaux de groupe. Lors de l’immersion, les étudiants sont encadrés par des professionnels de santé jouant le rôle de tuteurs, tandis que les enseignants facilitent les discussions et la réflexion critique. Une approche collaborative et participative est privilégiée pour impliquer activement les étudiants. Le projet repose sur des immersions en petits groupes, permettant aux étudiants d’interagir avec les membres de l’équipe interprofessionnelle, les patients et leurs familles. L’évaluation de la formation immersive en soins palliatifs a été réalisée à l’aide d’un questionnaire en ligne fondé sur le modèle de Kirkpatrick pour l’évaluation des programmes éducatifs (Niveau 1 : Réaction). Résultats 21 étudiantes ont évalué l’immersion clinique. 4 étudiants de médecine et 17 étudiants en soins infirmiers. Tous les résultats ont dépassé 4,5 sur une échelle de 1 à 5, témoignant d’une forte approbation de l’expérience immersive. Conclusion Les expériences cliniques immersives en soins palliatifs s’avèrent efficaces pour combler le fossé entre théorie et pratique chez les étudiants en médecine et en soins infirmiers. Ce modèle pédagogique favorise non seulement le développement des compétences cliniques, mais aussi la collaboration interprofessionnelle et une approche globale centrée sur le patient et ses proches. |
||
|
P3
DigiPall: Translating Digital Healthcare Innovation into Clinical Practice for Palliative Care
Manuel Amann, Zürich CH
Abstract
Hintergrund
The translation of digital health technologies from concept to clinical implementation faces significant barriers, particularly in vulnerable populations such as palliative care patients. Systematic evaluation frameworks are essential for successful technology adoption in healthcare settings. Ziel To demonstrate how structured testing environments can accelerate the development of evidence-based digital health interventions, using the progression from the Wearable Workbench platform to the DigiPall clinical trial as a case study. Methode The Wearable Workbench initiative (2023) established a standardized testing environment for palliative care technologies, evaluating nine wearable devices and ten chatbot platforms using validated instruments including the User Experience Questionnaire and System Usability Scale. Patient-centered testing with actual palliative care recipients informed technology selection and refinement processes. Resultate DigiPall represents a refined digital intervention combining validated components: the Corsano CardioWatch 287-2 for continuous physiological biomarker capturing and a WhatsApp-based chatbot for daily symptom assessment. The intervention delivers personalized daily check-ins, adaptive symptom management guidance, and continuous biomarker capture to enhance patients’ sense of security while maintaining home-based care. The aim is to address the critical gap in palliative healthcare where up to 50% of emergency visits are potentially avoidable. A randomized controlled trial (n=382) will evaluate DigiPall's effectiveness in reducing unplanned hospitalizations among palliative care patients while measuring impacts on quality of life and sense of security. The Wearable Workbench generated systematic evidence on technology usability, acceptability, and technical feasibility in palliative care settings. This foundation enabled rapid development of DigiPall, significantly reducing development time and costs through established evaluation frameworks and component validation. Schlussfolgerung The Wearable Workbench's role as both testing platform and methodology repository demonstrates how structured innovation pathways in digital health can successfully transform exploratory concepts into evidence-based clinical interventions. This progression exemplifies effective translation of user-centered design principles into digital health solutions for vulnerable populations. |
||
|
P4
Identification and team consultation of patients with complex palliative care needs in internal medicine wards
Antonella Avena, Bellinzona CH
Abstract
Contexte
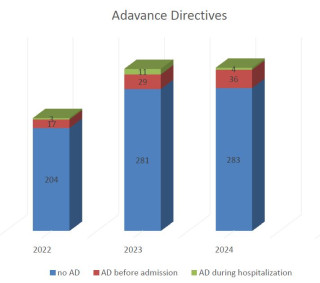
Several studies have shown that palliative care (PC) improves symptom management, shared-decision making, and overall quality-of-life of patients and their families. Patients hospitalised in internal medicine wards are at risk of unjust access to PC services, as their needs are often under recognised. Therefore, we developed an innovative consultation model, where multidisciplinary PC teams are providing integrated care within internal medicine wards in our multicentre institution. Objectiv Evaluate the impact of an integrated consultation model on healthcare professionals’ identification of patients requiring specialised PC. Méthode Retrospective observational study conducted from January 2022 to December 2024 in two internal medicine wards with integrated PC consultations. Included patients were adults ≥18 years with a life-limiting condition. Healthcare professionals identified PC recipients through a validated tool (ID-PALL), for the use of which were previously trained in small interdisciplinary groups. Demographics and data were collected in coded form on a duly created database. Descriptive statistics supported data analysis. Résultats In 2022,224 patients were identified and treated as patients with specialized PC needs patients in both internal medicine wards. These numbers increased rapidly over 12 months, with 321 patients identified in 2023 and the overall trend was confirmed in 2024, with 319 patients. Within this population, also the proportion of non-oncological life-limiting conditions increased (39% in 2022, 42% in 2023 and 41% in 2024). Similarly to what is known from the literature, a small percentage of patients had advance directives (AD) at the time of admission (17 in 2022, 29 in 2023 and 36 in 2024) and at discharge only a small number of AD discussion were accomplished. Conclusion Early identification of patients in needs for specialised PC fosters shared decision-making about further treatments and goals for the future. Supporting awareness in internal medicine wards about PC needs helps to provide specialised PC where patients are hospitalised. Future research plans include evaluation of staff perceptions and benefit of our integrated PC consultation and strategies to increase discussions on AD during the hospitalisation. 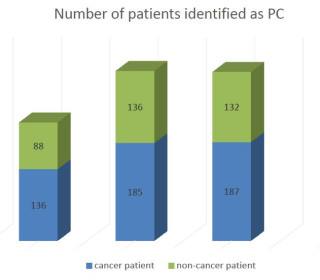
|
||
|
P5
Etat des lieux de la prise en charge palliative dans les services de réanimation en Algérie
CHABANE Baidi, BECHAR DZ
Abstract
Contexte
L’Algérie, en tant que pays émergent, fait face à une transition épidémiologique caractérisée par une prévalence croissante des maladies chroniques et dégénératives. Cette évolution engendre des défis majeurs en matière de santé publique, notamment en ce qui concerne la prise en charge des patients en phase terminale. Les soins palliatifs, qui visent à améliorer la qualité de vie des patients confrontés à des maladies graves, évolutives ou terminales, constituent une réponse essentielle à ces défis. Traditionnellement, les services de réanimation en Algérie sont orientés vers la lutte contre la mort, avec pour objectif principal de sauver des vies. Cependant, face à des situations où les options thérapeutiques curatives sont épuisées, l’intégration des soins palliatifs devient cruciale pour soulager la souffrance des patients et accompagner leurs familles. C’est dans ce contexte que l’Établissement Hospitalier Universitaire (EHU) “1er Novembre 1954” d’Oran a inauguré, en novembre 2018, la première unité de soins palliatifs du pays. Cette unité, dotée d’une capacité de neuf lits, est gérée par une équipe pluridisciplinaire composée de médecins spécialistes, de généralistes, de paramédicaux et de psychologues. Elle offre une prise en charge globale, incluant le soulagement de la douleur physique et psychique, l’accompagnement des familles et des services d’hospitalisation à domicile . Malgré cette avancée, les soins palliatifs en Algérie restent en phase de développement. La nécessité d’une structuration nationale, d’une formation spécialisée du personnel médical et paramédical, ainsi que d’une sensibilisation accrue du public et des professionnels de santé, est impérative pour répondre efficacement aux besoins croissants en matière de soins palliatifs. Objectiv L’objectif est de recueillir des données permettant un état des lieux de la prise en charge palliative dans les unités de soins critiques. Méthode Il s'agit d'une étude observationnelle de type transversal, basée sur un questionnaire destiné à évaluer la prise en charge de la douleur et l'accompagnement des patients en soins palliatifs. Ce questionnaire sera adressé à l'ensemble des praticiens des services de réanimation médicale en Algérie. Les axes principaux abordés dans le questionnaire sont :
L’objectif est de recueillir des données permettant un état des lieux de la prise en charge palliative dans les unités de soins critiques. Questionnaire sur la douleur et les soins palliatifsDans le cadre de cette étude, un questionnaire a été élaboré afin d’évaluer la perception des soignants et des patients quant à la prise en charge de la douleur en soins palliatifs. Ce questionnaire comprend plusieurs volets :
o Profession : aide-soignant, infirmier, médecin, autre o Années d’expérience dans le service o Formation spécifique en soins palliatifs (oui/non)
o Échelle d’évaluation de la douleur utilisée (EVA, échelle verbale, échelle faciale, etc.) o Fréquence d’évaluation de la douleur o Difficultés rencontrées dans l’évaluation de la douleur (communication, subjectivité, etc.)
o Traitements antalgiques prescrits (palier 1, 2 ou 3 selon l’OMS) o Utilisation des thérapeutiques non médicamenteuses (relaxation, accompagnement psychologique, etc.) o Accès à la morphine ou autres opioïdes
o Présence d’un accompagnement psychologique o Implication des familles dans la prise en charge o Protocoles institutionnels pour l’accompagnement en fin de vie
o Besoins en formation o Manque de moyens ou de protocoles spécifiques o Nécessité d’une meilleure coordination pluridisciplinaire Ce questionnaire a pour objectif de dresser un état des lieux des pratiques et des représentations liées à la gestion de la douleur en contexte palliatif, afin d'identifier les axes prioritaires d'amélioration dans le système de santé algérien. Résultats Résultats attendus (en cours)Cette étude vise à atteindre les objectifs suivants : · Déterminer les méthodes les plus utilisées pour évaluer la douleur en réanimation. · Identifier les pratiques courantes en matière de prise en charge de la douleur. · Évaluer la place et l’intégration des soins palliatifs dans les services de réanimation. · Recueillir les besoins exprimés par les soignants pour améliorer la qualité des soins palliatifs. · Mettre en évidence les freins institutionnels et logistiques à une meilleure prise en charge palliative. Discussion L’impact attendu de ce questionnaire, permet d’anticiper les lacunes majeures dans la gestion de la douleur et l’accompagnement en fin de vie. Il mettra en lumière les besoins en formation, la faible accessibilité à certains traitements comme les opioïdes, ainsi que le manque de protocoles spécifiques dans les services de réanimation. Il offrira également une base pour des recommandations ciblées en vue d’un développement cohérent et éthique des soins palliatifs en Algérie, adaptés aux réalités locales. Cette étude s’inscrit dans une démarche d’amélioration continue de la qualité des soins, en intégrant la voix des soignants confrontés quotidiennement aux limites curatives de la médecine. Conclusion Cette étude transversale, fondée sur un questionnaire adressé aux professionnels de la réanimation médicale en Algérie, s’inscrit dans une volonté d’explorer les pratiques actuelles en matière de soins palliatifs, et plus particulièrement de prise en charge de la douleur et d’accompagnement en fin de vie. Elle vise à identifier les pratiques, les besoins et les insuffisances existantes, dans un contexte où la médecine algérienne est encore en phase de structuration sur ce sujet. Les résultats attendus permettront de dresser un état des lieux des connaissances, des représentations et des moyens mobilisés dans les services de réanimation, face à la souffrance des patients en phase terminale. Cette initiative, bien que localisée, peut constituer une base de réflexion nationale, d’autant plus que l’Algérie, à l’instar de nombreux pays émergents, considère encore la prise en charge palliative comme un champ en devenir. Ainsi, il apparaît indispensable de renforcer la structuration des soins palliatifs à travers l’instauration d’un cadre législatif clair, la mise en place de référentiels institutionnels adaptés, et la promotion d’une culture médicale intégrant les dimensions éthique, humaine et scientifique du soin en fin de vie. Cela suppose également de développer des formations spécialisées et continues à destination des soignants, ainsi que de favoriser la recherche clinique dans ce domaine encore peu investi. Une telle dynamique permettrait d’ancrer durablement les soins palliatifs dans la stratégie nationale de santé et de garantir à chaque patient une prise en charge digne, humaine et scientifiquement fondée, même lorsque la guérison n’est plus possible. |
||
|
P6
Gedanken zum Lebensende älterer Menschen durch Erzählkunst und Theater: eine qualitative Studie
Eleonore Baum, St.Gallen CH
Abstract
Hintergrund
Das Lebensende ist ein Thema von grosser Relevanz, besonders für ältere Menschen, deren Bedürfnisse und Herausforderungen oft unzureichend berücksichtigt werden. Ziel Ziel der Studie ist es, ihre Perspektiven zu diesem Thema zu erfassen und einen Beitrag zur Verbesserung der Palliative Care zu leisten. Im Fokus stehen Herausforderungen wie eingeschränkter Zugang zu Unterstützungsangeboten, alters- und geschlechtsbedingte Ungleichheiten sowie gesellschaftliche Tabus, die den Umgang mit dem Lebensende erschweren. Diese Barrieren führen zu verzögerter Versorgung und suboptimaler Betreuung. Methode Diese multimethodische qualitative Studie nutzt kreative Ansätze, um ältere Menschen in Diskussionen über das Lebensende einzubeziehen. Dazu gehören Erzähl-Cafés (mindestens drei Veranstaltungen, in denen persönliche Erfahrungen geteilt und kollektive Perspektiven entwickelt werden), Improvisationstheater-Workshops (mehrere kreative Workshops in einem Pflegeheim, moderiert von einer Theaterpädagogin) und Playback-Theater (aufgeführt durch Laienschauspieler in einer öffentlichen Einrichtung durch Einbezug von Geschichten der Zuschauenden zum Lebensende). Ergänzend werden Familieninterviews durchgeführt, um die Perspektiven älterer Menschen und ihrer Angehörigen zu vertiefen. Die Datensammlung erfolgt durch Feldnotizen, Beobachtungen, Protokolle und Transkripte. Die Auswertung orientiert sich an der thematischen Inhaltsanalyse und bezieht relevante Interessengruppen zur Validierung ein. Resultate Die Zwischenanalyse zeigt, dass die Kombination klassischer und kreativer Methoden zu einem tiefergehenden Verständnis der Gedanken älterer Menschen bezüglich des Lebensendes führt. Insbesondere betonen die Ergebnisse die Bedeutung von Unterstützungsnetzwerken, Lebensumständen und individuellen Faktoren, die die Wahrnehmung und Erfahrungen älterer Menschen prägen. Schlussfolgerung Die ersten Erkenntnisse unterstreichen die Notwendigkeit, Palliative Care stärker an den gelebten Erfahrungen und Werten älterer Menschen auszurichten. Durch die Integration kreativer Ansätze kann nicht nur das öffentliche Bewusstsein für Themen des Lebensendes geschärft werden, sondern es entstehen auch neue Möglichkeiten für Dialog und Reflexion in der Gemeinschaft. Die Studie bietet Einblicke, die Impulse für eine einfühlsamere und stärker auf die Bedürfnisse älterer Menschen abgestimmte Palliative Care setzen können, insbesondere durch den Einsatz innovativer Ansätze. 

|
||
|
P7
Palliative Care für Menschen mit kognitiver Beeinträchtigung in der Ostschweiz (Projekt PAL_LINK)
Daniela Bernhardsgrütter, St.Gallen CH
Abstract
Hintergrund
Erhebungen in der Schweiz zeigen, dass die Zahl der Menschen mit kognitiven, körperlichen oder psychischen Beeinträchtigungen, welche 55 Jahre und älter werden, wächst. Damit einher geht die steigende Prävalenz chronischer und altersbedingter Erkrankungen sowie der zunehmende Bedarf an Palliative- und End-of-Life-Care. Dennoch existieren in der Schweiz bislang keine übergreifenden Versorgungskonzepte, die Menschen mit kognitiver Beeinträchtigung, Fachpersonen und Angehörige im Umgang mit Palliative- und End-of-Life-Care-Bedürfnissen unterstützen. Ziel Das Projekt PAL_LINK hat zum Ziel, ein Konzept für die Palliative- und End-of-Life-Care-Versorgung von Erwachsenen mit kognitiver Beeinträchtigung in der Ostschweiz zu entwickeln. Methode Das laufende Praxisentwicklungsprojekt (2024–2027) schliesst Personen mit kognitiver Beeinträchtigung, ihre Angehörigen und Fachpersonen partizipativ in den Entwicklungsprozess mit ein und gliedert sich in zwei Phasen:
Resultate Die Analyse von 483 Fragebögen, 7 Einzel- und Gruppeninterviews und einem Workshop zeigen bedeutsame Unterschiede zwischen den Institutionen für Menschen mit kognitiver Beeinträchtigung in der Ostschweiz. Diese Unterschiede betreffen sowohl institutionelle Rahmenbedingungen (z.B. Finanzierungsstrukturen) als auch das Wissen und die Kompetenzen des Fachpersonals im Umgang mit Palliative- und End-of-Life-Care-Bedürfnissen. Ein auf unterschiedlichen Ebenen wiederkehrendes Thema ist der nicht strukturell verankerte interprofessionelle Austausch zwischen Fachpersonen aus der Pflege und der Sozialen Arbeit. Schlussfolgerung Einzelne Institutionen weisen bereits etablierte Prozesse auf hinsichtlich der Versorgung von Menschen mit kognitiver Beeinträchtigung am Lebensende. Insgesamt zeigen die Ergebnisse jedoch, dass das Bewusstsein und das Wissen zum Thema noch sehr fragmentiert sind. Die Etablierung eines interprofessionellen und institutionsübergreifenden Versorgungskonzepts und Netzwerks ist deshalb essenziell. |
||
|
P8
Financial Distress in der geriatrischen Palliative Care – eine Multimethoden-Studie (FinStress_Pal)
Daniela Bernhardsgrütter, St.Gallen CH
Abstract
Hintergrund
Finanzielle Sorgen im Alter sind eine gegenwärtige Herausforderung in der Schweiz, insbesondere in der pflegeintensiven letzten Lebensphase. Nationale und internationale Studien und der Austausch mit Expertinnen und Experten zeigen auf, dass die Bewältigung finanzieller Angelegenheiten für ältere Menschen am Lebensende ein zentrales Bedürfnis darstellt. Neben früheren wirtschaftlichen Einbussen spielen altersspezifische Faktoren eine zentrale Rolle. Finanzielle Sorgen („finanzieller Distress“) betreffen jedoch nicht nur die objektiven Kosten, sondern auch die subjektive Wahrnehmung der Betroffenen und Angehörigen. Im Gegensatz zu den objektiven Kosten fehlt es an Studien, wie ältere Menschen mit Palliative Care Bedarf sowie ihre Angehörigen finanziellen Distress erleben und wie dies die Nutzung formeller und informeller Pflege- und Betreuungsdienste beeinflusst. Ziel Das Ziel des Projekts ist es, 1) Erfahrungen mit finanziellem Distress bei älteren Menschen mit Palliative Care Bedarf sowie deren Angehörigen explorativ zu untersuchen; 2) die Wechselwirkungen von finanziellem Distress und gesundheitsrelevanten Variablen zu modellieren; und 3) das Thema «finanzieller Distress in der geriatrischen Palliative Care» zu enttabuisieren. Methode Das Projekt (2025-2027) verfolgt ein multimethodisches Forschungsdesign: 1) Multiple Case Study; 2) systematische qualitative Übersichtsarbeit; 3) Synthese und modellhafte Darstellung der Erkenntnisse mittels partizipativem «system dynamics»-Ansatz; 4) Entwicklung von Tools, die als Türöffner zur Sensibilisierung und Enttabuisierung von finanziellem Distress in der geriatrischen Palliative Care dienen. Resultate Zurzeit wird die Datenerhebung der Multiple Case Study durchgeführt. In der systematischen Übersichtsarbeit konnten 13 qualitative Studien eingeschlossen werden. Die Ergebnisse verdeutlichen die hohe Relevanz und die Konsequenzen von sozialen und wirtschaftlichen Ressourcen am Lebensende. Dabei spielen beispielsweise die Aufteilung konkreter pflegerischer Tätigkeiten innerhalb der Familie oder ein unterstützendes Arbeitsumfeld eine wichtige Rolle. Schlussfolgerung Ältere multimorbide Menschen werden in Zukunft die Hauptempfängerinnen und -empfänger von Palliative Care sein. Die Auseinandersetzung mit den ganzheitlichen Bedürfnissen dieser vulnerablen Personengruppe und ihrer Angehörigen – zu denen auch ihre finanziellen Sorgen zählen – liefert entscheidende Impulse für die Weiterentwicklung einer qualitativ hochstehenden geriatrischen Palliative Care. |
||
|
P9
Early Integration of Palliative Care in the Treatment of Women with Advanced Breast or Gyn. Cancer
Esther Birindelli, Zurich CH
Abstract
Hintergrund
Patients with advanced breast and gynecological cancers now live longer due to improved treatment options but often experience complex and evolving symptom burdens. Traditional outpatient oncology care may not fully meet their physical, emotional, or social needs. To promote early integration of palliative care, a joint outpatient consultation was established in 2023, co-led by a physician and a nurse practitioner with expertise in gynecologic oncology, breast cancer and palliative care (GynOnc/BC/PC). Ziel This project studies patients’ emotional functioning following a joint outpatient consultation with GynOnc/BC/PC multidisciplinary specialists. A secondary goal is to assess caregiver burden. Methode A Phase II single-arm pre-post study is underway to evaluate changes in patients' emotional functioning following the GynOnc/BC/PC consultation. The study includes 35 consecutively recruited patients and 11 caregivers. The primary endpoint is the change in emotional functioning at 6 weeks after initial consultation, measured using the EORTC QLQ-C15-PAL. Secondary outcomes include symptom burden, assessed by the Integrated Palliative Outcome Scale (IPOS) and unmet palliative care needs. Patients complete questionnaires at baseline, 6, 12, and 24 weeks. Caregivers complete the Zarit Burden Interview at the same intervals. Data on hospital admissions and consultations are extracted from medical records. The consultation focuses on symptom management, decision-making support, prognosis communication, and care planning. Patients are offered a follow-up consultation after 12 weeks. Results will be analyzed using Wilcoxon signed-rank tests and descriptive statistics. Resultate This ongoing study includes a planned interim analysis in early 2026. Diskussion The findings will inform future care models for patients with advanced breast and gynecologic cancers. Early palliative care involvement can reduce suffering for patients, improve informed decision-making, and increase care alignment with patient values. It may also enhance system efficiency by reducing emergency visits and avoidable hospitalizations. Supporting caregivers helps them manage emotional, physical, and financial stress, contributing to overall care stability. Schlussfolgerung This study will generate small-scale yet valuable insights into the early integration of palliative and gynecologic oncology/breast cancer care. In doing so, it contributes to the evidence base for innovative interdisciplinary models of service delivery in palliative care. |
||
|
P10
“Not at home”: insights from case studies on setting preferences in assisted suicide
Claudia Gamondi, Lausanne CH
AbstractContexte In Switzerland, limited access to assisted suicide in hospitals and nursing homes results in approximately 76% of procedures taking place at home and only two university hospitals permit the procedure to occur within their facilities. In some instances, individuals are sent back to their homes to complete the final act, despite a stated preference for a hospital setting. Although individuals might initially express a preference to die at home, the realities of undergoing assisted suicide at home can challenge,(or even reverse) that preference. Such situations raise complex ethical issues around autonomy and respect for personal preferences. However, it has been very little addressed in research and individuals' expressed preferences for the location of assisted suicide remains limited. Investigating how people experience the home environment during this process is essential to understand how it may, in some cases, shift from a preferred to an undesired place to die. Objectiv To describe individuals’ concerns about undergoing an assisted suicide at home and to explore individuals’ perception of safety during the procedure. Méthode Four "extreme" cases studies were selected from a sample of 27 participants. We conducted in-depth semi-structured interviews with individuals and their relatives, at home. Data was analyzed through thematic analysis. Résultats The four case studies reveal four concerns associated to home-based AS: compromised efficiency, security and management of the procedure, lack of care and support, emotional impact on the family, and being confronted with personal memories & home environment. These factors were linked to significant difficulties for both family members and the decision-maker and reflect the individuals’ perception of elements associated to feeling safe. Conclusion These results underscore the importance of the location in the request for assisted suicide. They reveal that undergoing assisted suicide at home can create substantial challenges, prompting some individuals to prefer hospital-based procedures. This study offers valuable insights for further ethical discussions on respecting individuals’ preferences, and feeling of safety, in assisted suicide. |
||
|
P11
Implementierung des ESAS-r in der stationären Langzeitpflege: Herausforderungen und Lösungsansätze
Rouven Brenner, Stäfa CH
Abstract
Hintergrund
Hintergrund: Langzeitpflegeinstitutionen leisten einen essenziellen Beitrag in der Grundversorgung von älteren Menschen mit Bedarf an allgemeiner Palliative Care. Im Rahmen der Zertifizierung in allgemeiner Palliative Care wurde das überarbeitete Edmonton Symptom Assessment System (ESAS-r) im Alterszentrum Lanzeln implementiert. Ziel Ziel/Forschungsfrage: Im Mittelpunkt der Untersuchung stand die Frage, wie das ESAS-r trotz settingspezifischer Herausforderungen, wie Schwierigkeiten bei der Identifikation geeigneter Zielgruppen oder fehlender objektiver Anhaltspunkte für Fremdeinschätzungen durch Pflegekräfte, nachhaltig in der stationären Langzeitpflege etabliert werden kann. Methode Methoden: Es wurde eine systematische Literaturrecherche in pflegerelevanten Datenbanken durchgeführt, um bestehende Evidenz zur Implementierung von ESAS-r zu sammeln. Ergänzend wurden Kontakte zu erfahrenen Anwendern und der Originalautorin des ESAS-r aufgenommen. Workshops mit Mitarbeitenden wurden abgehalten, um zusätzliche objektive Kriterien für die Fremdeinschätzung von Symptomen zu entwickeln. Die Implementierung erfolgte anschliessend in mehreren Phasen, begleitet von einer kontinuierlichen Evaluation. Resultate Resultate: Bereits in der Vorbereitungsphase zeigte sich, dass eine routinemässige Anwendung des Instruments bei allen Bewohnenden als zu belastend wahrgenommen wurde. Daher wurde ein bestehender Algorithmus zur Bestimmung der Symptomkomplexität (nach Watson et al., 2020) angepasst, um die Zielgruppe präzise zu definieren: Bewohnende in der End-of-Life-Care-Phase und/oder mit moderater bis schwerer Symptomkomplexität. Zudem wurden spezifische, objektivierbare Kriterien für die Fremdeinschätzung verschiedener Symptome, wie Müdigkeit, Übelkeit, Angst oder Atemnot, entwickelt und implementiert. Schlussfolgerung Schlussfolgerung: Auch bewährte Assessmentinstrumente aus dem Bereich der spezialisierten Palliative Care erfordern eine Anpassung an das jeweilige Setting und die spezifische Population in der stationären Langzeitpflege. Die Implementierung des ESAS-r verbesserte die Symptomerfassung und -kontrolle insgesamt, wobei insbesondere Bewohnende mit kognitiven Beeinträchtigungen von der optimierten Fremdeinschätzung profitierten. Die erarbeiteten objektiven Kriterien sowie der angepasste Algorithmus bieten eine solide Grundlage für zukünftige Implementierungen. Für belastbare Aussagen ist jedoch eine weitere pflegewissenschaftliche Evaluation der Anpassungen notwendig. |
||
|
P12
Introduction d’une typologie des pratiques sédatives à visée palliative en fin de vie (SEDAPALL) dans une USP
Marion Broucke, Blonay CH
Abstract
Contexte
La sédation palliative recouvre une multitude de pratiques qui répondent à des situations cliniques complexes et diverses. Le recours à ce terme générique entraîne des confusions et/ou entretient une certaine ambiguïté autour des objectifs poursuivis, notamment en termes d’intentionnalité. Contrairement aux idées reçues, la sédation palliative ne se résume pas à la seule sédation profonde et continue maintenue jusqu’au décès. Objectiv Dans le cadre de l’amélioration des pratiques en soins palliatifs, ce projet visait à introduire une typologie validée en langue française (SEDAPALL) dans la procédure "sédation" de l’institution. L’objectif est de clarifier les pratiques sédatives, de favoriser un langage commun et de systématiser la réflexion pluriprofessionnelle avant de débuter toute sédation, autour de trois axes : durée envisagée (transitoire, indéterminée, maintenue jusqu’au décès), profondeur souhaitée (proportionnée ou profonde d’emblée), et consentement du patient (absent, anticipé, exprimé, ou demande explicite). Méthode Une présentation de l’outil SEDAPALL a été réalisée par l’infirmière clinicienne auprès de l’équipe interdisciplinaire. Cet outil structurant, inspiré des recommandations de la SFAP, permet une classification explicite des pratiques sédatives selon les trois dimensions mentionnées. La démarche s’est accompagnée d’un travail collectif de révision de la procédure institutionnelle, incluant des discussions cliniques, l’élaboration d’un suivi spécifique dans le dossier patient informatisé (DPI) et la mise en place de protocoles d’urgence adaptés. Résultats La révision intégrale de la procédure "sédation palliative" a été effectuée. Des protocoles d’urgence ont été élaborés et mis en place. L’équipe a progressivement intégré un langage commun, conduisant à une homogénéité des pratiques et une optimisation des prises en soins. La typologie SEDAPALL a permis une meilleure anticipation, une traçabilité rigoureuse et une adaptation plus fine des interventions sédatives au cas par cas. Discussion La typologie SEDAPALL a facilité l’alignement des intentions thérapeutiques avec les prescriptions sédatives. Elle a servi d’outil d’aide à la prise de décision tout en soutenant la collégialité et la transparence des pratiques. La classification (ex. : sédation transitoire, profonde d’emblée avec consentement du patient donné par anticipation) permet une communication claire entre soignants et avec les proches, et limite ainsi les risques de confusion entre sédation palliative et autres pratiques (anxiolyses, pratiques euthanasiques…). Elle répond avec précision aux besoins spécifiques de chaque patient dont l’état nécessite un recours à la sédation. Conclusion Ce projet a permis d’affiner la réponse thérapeutique face aux symptômes réfractaires en fin de vie, dans le respect des bonnes pratiques et du souhait des patients. L’implantation de la typologie SEDAPALL représente une avancée concrète pour structurer les pratiques sédatives, garantir la qualité et la sécurité des soins, et renforcer la réflexion éthique et collégiale en soins palliatifs. 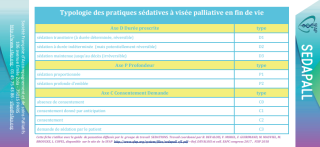
|
||
|
P13
Subkutane Verabreichung von Pantoprazol: eine prospektive Kohortenstudie auf einer Palliativstation
Cristian Camartin, Chur CH
Abstract
Hintergrund
In fortgeschrittenen Krankheitsstadien leiden Patienten häufig unter Schluckbeschwerden. In solchen Fällen ist die subkutane Medikamentengabe eine Möglichkeit und ein häufig genutzter Ansatz in der Palliativversorgung. Im klinischen Alltag kann eine breite Palette von Präparaten eingesetzt werden. Protonenpumpenhemmer (PPI) sind die Behandlung der Wahl bei verschiedenen gastrointestinalen Erkrankungen und zeigen eine hohe Wirksamkeit. Bei Patienten mit gastroenterologischen Symptomen wie Refluxösophagitis, Magengeschwüren und gastrointestinalen Blutungen besteht eine Indikation für den Einsatz von PPI. Auch können sie bei gastrointestinaler Obstruktion die Symptome lindern. Aufgrund des alkalischen pH-Werts ist die subkutane Gabe von PPI jedoch nicht etabliert. Dennoch können zahlreiche Medikamente im Off-Label-Use mit guter Wirkung und Verträglichkeit subkutan angewendet werden. Ziel Ist die subkutane Gabe von Pantoprazol als Off-Label-Use eine sichere Option bei Schluckbeschwerden? Können die Symptome erfolgreich behandelt werden? Methode Diese prospektive monozentrische Kohortenstudie wurde von Mai 2024 bis April 2025 auf einer spezialisierten Palliativstation durchgeführt. Wir verabreichten Patienten mit entsprechender Indikation, die nicht in der Lage waren Medikamente oral einzunehmen, subkutan Pantoprazol. Die Zubereitung bestand aus 40 mg Pantoprazol, verdünnt in 50 ml 0.9 %iger Natriumchloridlösung und wurde als kontinuierliche subkutane Infusion über 30 Minuten mit Hilfe einer Infusionspumpe über eine 22-G-Kanüle verabreicht. Subjektive Symptome, objektive lokale Reaktionen und Behandlungseffekte wurden während des gesamten Verabreichungszeitraums beobachtet und dokumentiert. Das Medikament wurde einmal täglich verabreicht, bis der Patient die Fähigkeit zur oralen Einnahme wiedererlangte oder bis er verstarb. Resultate Insgesamt 18 Patienten (6 Männer und 12 Frauen) mit einem Durchschnittsalter von 68.6 Jahren (52–85 Jahre) wurden über einen Zeitraum von 1 bis maximal 19 Tagen behandelt. Die durchschnittliche Anwendungsdauer betrug 7.6 Tage. Die häufigste Indikation war eine gastrointestinale Obstruktion (10 Fälle). 5 Patienten wurden wegen gastrointestinaler Blutungen behandelt. Seltenere Indikationen waren Reflux und Darmperforation; jeweils ein Patient wurde behandelt. Die Grunderkrankung war bei 15 Patienten eine fortgeschrittene Tumorerkrankung, während Sepsis, Leberzirrhose und Divertikulitis bei jeweils einem Patienten die primären Erkrankungen waren. Subjektiv wurden die Symptome der Patienten erfolgreich behandelt. Objektiv trat in zwei Fällen nach Schlussfolgerung Die subkutane Gabe von Pantoprazol ist eine sichere Option und kann bei Palliativpatienten zur effektiven Behandlung gastrointestinaler Symptome eingesetzt werden. Lokale Reaktionen wie leichte Schmerzen und Rötungen können gelegentlich auftreten. Bei Schluckbeschwerden ist die tägliche subkutane Gabe mittels kontinuierlicher subkutaner Infusion über 30 Minuten eine sinnvolle Option. |
||
|
P14
Keta-Care - Antidepressant and anxiolytic effects of intranasal ketamine in palliative care patients
Ian Clark, Zürich CH
Abstract
Hintergrund
Ketamine is frequently used off-label intravenously in palliative care (PC) settings to manage anxiety and depression, common and highly distressing symptoms experienced by patients with terminal illness. Intranasal ketamine is a minimally invasive alternative to intravenous administration, with faster onset than monoaminergic antidepressants showing good tolerability. Evidence of antidepressant and anxiolytic effects, including safety of low-dose intranasal ketamine in this vulnerable population derives mainly from case studies with small samples, and off-label use is thus based principally on clinician experience. We aim to systematically evaluate the effects and feasibility of low-dose intranasal ketamine to treat acute anxiety and depression in a larger PC patient sample. Ziel The study is designed as collaborative open-label feasibility study in the intersection of oncology, psychiatry and palliative care, with the primary aim of assessing the benefit of intranasal ketamine applications on depression and anxiety in a palliative care out-patient setting over a time-period of 8 weeks per study patient. The secondary aim is to assess the burden of quality of life of patient caregivers to identify potential benefits of the IMP on caregivers. Methode Fifty PC patient-caregiver dyads will be recruited. Intranasal ketamine will be self-administered open-label by patients under supervision once per week for 8 weeks dosed flexibly (5 - 50 mg). Outcomes will be assessed at each administration. Primary outcome is change from week 1 to week 8 in Montgomery-Asberg Anxiety Depression Rating Scale. Secondary outcomes in patients include Hamilton Anxiety Rating Scale, Hospital Anxiety Depression Scale and in caregivers Zarit Burden Scale and CareGiver Oncology Quality of Life Questionnaire. Patient safety outcomes include acute side effects and adverse events. Resultate We hypothesize a statistically significant change in average scores of primary and secondary outcomes at week 1 compared to at week 8 indicating intranasal ketamine benefit. Rate of adverse events is hypothesized not to exceed the average rate of adverse events of the PC population. Schlussfolgerung Treatment of anxiety and depression with ketamine reflects a sea change in thinking about antidepressant and anxiolytic pharmacology with potential to be the new standard treatment for anxiety and depression in PC settings, given sufficient evidence for feasibility and safety, which this study protocol aims to generate. |
||
|
P15
Developing a support program for family caregivers during end of life at home
Nina Canova, Yverdon-les-Bains CH
Abstract
Contexte
Swiss healthcare policy promotes end-of-life care at home, reflecting the wishes of citizens and decreasing healthcare spending. Dying at home represents a challenge for both the health and social care network and for the family caregivers who risk physical, mental, and social difficulties even after death of their loved one. Support is available but remains limited in addressing death and bereavement and lacks a proactive approach and coordination. Objectiv The aim of the Confidence in End-Of-Life CAREgiving (CEOL-CARE) project was to develop with stakeholders, an intervention to strengthen the confidence of family caregivers and the network to better support a person at the end of life at home, including the early bereavement phase. Méthode The project was led by the Palliative and Supportive Care Service of Lausanne University Hospital in collaboration with the School of Management and Engineering Vaud, University Hospital Berne, and University College Dublin. A participatory action research method was used involving family caregivers, and associated care organizations. Résultats A nurse-led intervention has been developed which supports the family caregiver during the end-of-life period and after the patient's death, structured into two main phases: before and after the patient's death, with strong emphasis on needs assessment and response, and bereavement follow-up. It provides guidance and tools to help family caregivers and professionals navigate a complex system of existing services, while also facilitating the coordination and integration of these resources. Conclusion The CEOL-CARE project is an innovative process that recognizes the knowledge developed by family caregivers in the same way as that gained by professionals. The intervention aims to help sick people realize their end-of-life wishes at home, by supporting both family caregivers and nurses. By facilitating the connection and use of already available resources, it also considers the limits of the healthcare system. The next stage, scheduled for 2026, will be to test and implement the program. A national roll-out is also envisaged. |
||
|
P16
Engagement in advance care planning: effect of the card game Anticip’action in a community setting
Christine Clavien, Genève CH
Abstract
Contexte
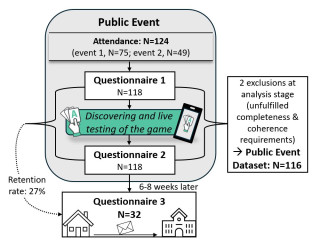
The card game Anticip'action was developed to foster Advance Care Planning (ACP) culture in medical and community settings. Available in a mobile (smartphone app) and paper formats, this conversation tool helps users to clarify and express their fears, hopes and life priorities, and to carry out actions in line with them. Objectiv The goals of this study were to (1) evaluate in a community setting, the effect of presenting Anticip’action on attitude towards ACP, self-perceived preparedness in case of adverse events, and action readiness, as well as to collect (2) users’ evaluation of the game, and (3) their preference to use the game in mobile or paper formats. Méthode Participants attended a 90-minute public event on the topic of advance directives, received information about ACP, filled questionnaire 1 (Q1), were introduced to the game, filled Q2, took the game home, and returned Q3 6-8 weeks later. Data collection included retention rates; pre-post responses on self-perceived preparedness in case of adverse events, attitude towards ACP, and readiness to take related actions (analyzed using paired Welch t-test on mean 1-5 Likert scores); proportions of anticipatory actions (planned or done) reported in Q3; average endorsement and perceived impact of the game (uMars, 1-5 Likert scores); proportions of reported intention and actual use of the game. Résultats Of the 124 attendees, 118 (mean age 75) completed Q1 & Q2, and 32 returned Q3. Baseline levels of attitude, self-perceived preparedness and readiness were uncommonly high (from 2.87 to 4.56). Discovering the game did not significantly impact these values. However, in Q3 (N=32), 72% of respondents reported intending to take one or several specific anticipatory actions, and 22% had accomplished at least one since discovering the game. Anticip’action obtained high endorsement scores (Q2=3.67, Q3=3.9) and was evaluated as highly impactful for fostering anticipation (Q2=4.19, Q3=4.17). At home, participants generally preferred using the paper version. Conclusion Anticip’action, especially in its paper format, is highly endorsed by a senior population with an existing interest in ACP and appears to effectively support the implementation of anticipatory actions. These findings need to be confirmed in larger and more diverse populations. 
|
||
|
P17
A conversation game to facilitate advance care planning in pediatrics
Christine Clavien, Genève CH
Abstract
Contexte
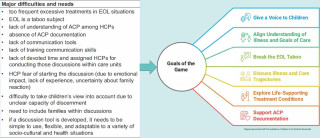
Advance Gare Planning (ACP) is rarely conducted in pediatric contexts or initiated too late and only with parents. ACP is too frequently associated with end-of-life care, although good practice advises to start the process earlier. Additionally, few child-friendly conversation tools exist to facilitate these sensitive discussions. Objectiv Our aim was to develop a conversation game to facilitate ACP discussions between healthcare professionals (HCPs), children aged 6 to 12, and their family caregivers.
Méthode
Résultats Results of 1st objective: 19 target articles, 31 responses to the questionnaires, 2 group consultations with experts, individual consultations with multiple experts and stakeholders. Major difficulties and needs and resulting goals of the game are detailed in Table1. Result of 2nd objective: L'Arbre (The Tree) is played in two separate sessions, first with the nurse and the adult family caregiver, then with the nurse and the child. Using the metaphorical language of the tree, it takes the form of a story in which children are the heroes and can talk about themselves. lt is structured into four stages of gameplay covering the topics of: 1) getting to know children 's family surroundings (e.g. their preferred caregivers) 2) understanding children s fears and hope 3) exploring perceptions of death or preferences for care in case of deteriorating health 4) exploring children s resources Conclusion The game offers a safe and caring environment that enables HCPs to address ACP topics with greater ease, empowers children and families to express their fears and values, and fosters patient centered decision-making in pediatric care. Usability and feasibility studies are ongoing to improve the game. 
|
||
|
P18
Projet de soins anticipé en dialyse: perspectives des patient.es et des professionnel.les
Gora Da Rocha Rodrigues, Lausanne CH
AbstractContexte Introduction : Le taux de morbidité et de mortalité des patient.e.s dialysé.e.s est élevé. Cependant, ils.elles bénéficient rarement de projet de soins anticipé (ProSA). Nous avons développé une intervention utilisant un jeu de cartes sérieux pour faciliter l'initiation de discussions sur le ProSA avec les patient.e.s dialysé.e.s par les infirmier.ère.s. Objectiv Les objectifs de cette étude étaient d'explorer les facilitateurs et les obstacles à l’implémentation ainsi que la valeur perçue de l'intervention. Méthode Des entretiens semi-structurés et des groupes de discussion ont été menés avec des patient.e.s, des infirmier.ère.s et des néphrologues après la phase d'intervention, entre décembre 2022 et décembre 2023. Résultats Au total, 15 patient.e.s, 13 infirmier.ère.s et 5 médecins ont participé à l'étude. Quatre thèmes ont été identifiés : (1) le contenu et le format de l'intervention ; (2) l'influence des caractéristiques des participant.e.s ; (3) l'intégration dans les soins généraux et (4) les résultats liés à l'intervention. Le jeu de cartes a permis aux patient.e.s d'acquérir une compréhension globale de leur état de santé, de leurs objectifs personnels et de leurs préférences en matière de traitement et de les partager avec leur.s proche.s, tout en fournissant aux infirmier.ère.s un cadre structuré pour initier les discussions sur le ProSA. La formation continue et les séances de supervision réflexive avec des accompagnateur.trice.s expérimenté.e.s en matière de ProSA ont permis aux infirmier.ère.s de délivrer l’intervention de manière confiante. Les principales difficultés relevées par les participant.e.s étaient liées aux facteurs individuels (ex : croyances personnelles) et organisationnels (ex : environnement, temps). Conclusion Cette étude qualitative soutient l'utilisation d'un jeu sérieux pour promouvoir les discussions sur le ProSA pour les patient.e.s dialysé.e.s. Les résultats de l’étude invitent à l’élaboration de nouvelles stratégies pour favoriser l’engagement des professionnel.le.s de la santé dans la démarche du ProSA et pour dépasser certaines barrières organisationnelles. |
||
|
P19
Le case management dans les soins palliatifs de Rive-Neuve.
katia de Vargas, Blonay CH
Abstract
Contexte
Le case management, ou gestion de cas, est une approche de coordination des soins centrée sur la personne, qui vise à assurer la continuité, la qualité et l’adéquation des prises en charge pour des personnes aux besoins complexes.
Objectiv Présenter la mise en œuvre du case management à travers quatre programmes spécifiques développés à Rive-Neuve, et en explorer l’impact concret à travers des illustrations cliniques et une évaluation interne. Méthode L’étude repose sur une analyse qualitative de quatre programmes structurant le case management à Rive-Neuve :
Ces dispositifs seront explorés à l’aide de vignettes cliniques illustratives, issues de situations rencontrées dans la pratique. En complément, un questionnaire d’évaluation sera diffusé auprès des professionnels de l’Institut, afin de recueillir leur perception de la plus-value du case management dans leur pratique quotidienne. Résultats L’analyse des vignettes et les retours du questionnaire mettront en lumière l’impact du case management sur la fluidité des parcours de soins, la coordination interdisciplinaire, et l’adaptation fine aux besoins évolutifs des patients. Les premiers retours montrent une perception positive de cet outil comme levier de cohérence et de soutien à la décision. Discussion La structuration du case management en programmes ciblés permet d’anticiper les transitions, de mieux intégrer les proches, et d’appuyer les équipes dans une prise en charge centrée sur la personne. Cette approche favorise également une communication plus claire et partagée entre les acteurs du soin. Conclusion Le case management, lorsqu’il est conçu comme une pratique organisée et intégrée, contribue à renforcer la qualité, la coordination et l’humanité des soins palliatifs. L’expérience de Rive-Neuve illustre son potentiel structurant et adaptable au service des patients et des professionnels. |
||
|
P20
Stratégies palliatives dans les insuffisances cardiaques terminales
Maria Delgado, La Chaux-de-Fonds CH
Abstract
Contexte
L’insuffisance cardiaque est une pathologie touchant un grand nombre de patients malgré les démarches de prévention. Les soins palliatifs sont un élément clé dans la prise en charge de ces patients, lorsque la maladie atteint son stade terminal. Les patients atteints de formes avancées présentent des symptômes de gestion délicate d’où l’intérêt d’initier un suivi par une équipe de soins palliatifs afin d’optimiser la prise en charge. Objectiv La gestion optimale des symptômes et l'amélioration de la qualité de vie sont une priorité pour la pathologie mentionnée et la typologie des patients cités. Nous rapportons les directives palliatives récentes et mettons l'accent sur la gestion des symptômes principaux chez les patients en insuffisance cardiaque terminale. Méthode Nous avons réalisé une analyse intégrative modifiée de la littérature afin de mettre l’accent sur les symptômes les plus fréquents et souligner l’importance d’intégrer de façon systématique et précoce des soins palliatifs dans la prise en charge. Résultats Cette approche doit prendre en compte un obstacle majeur, à savoir l’évolution imprévisible et progressive de la maladie, caractérisée par une alternance des épisodes de décompensation et des phases de stabilisation (évolution en palier). Grâce aux avancées pharmacologiques et technologiques, le pronostic de la maladie s’améliore et la phase terminale est retardée ce qui nécessite une adaptation de l’approche palliatives dans le parcours de soins. Conclusion La prise en charge optimale de l’insuffisance cardiaque chronique exige une approche mixte qui associe les moyens pharmacologiques, les interventions non pharmacologiques et un suivi régulier intégrant les soins palliatifs dès le stade initial de la maladie. L’instauration de soins palliatifs devra être considérée comme un complément et non une alternative. Cette collaboration permet la prise en charge précoce des symptômes, un soutien à la prise de décision, une optimisation de la communication portant sur la progression de la maladie et la fin de vie, une planification anticipée des soins et l’intégration des dimensions psychosociales et spirituelles. |
||
|
P21
Usability test of a conversation game to facilitate advance care planning in pediatrics
Tatiana Delieutraz-Petit, Genève CH
Abstract
Contexte
Advance care planning (ACP) discussions are increasingly recognized as an important component of adequate care. However, they involve considering worst-case and end-of-life scenarios which are difficult to address. Few conversation tools exist to facilitate these sensitive discussions. An inter-professional research team at Geneva University and HUG hospital, has developed a game (L’Arbre) to initiate these discussions with patients and their families. Objectiv Assess the usability of the first prototype of the game (design, user-friendliness, learnability, relevance, endorsement). Méthode
Résultats
Modifications: All problems can be addressed with 17 minor changes and prior training of healthcare professionals. Conclusion L’Arbre was positively assessed by users and has demonstrated a significant potential for improving ACP communication. Several areas for improvement were identified. A V2 is in production and training concept and material are developed to ensure effective integration into practice. 

|
||
|
P22
Die Lebensende-Doula – Eine innovative Ergänzung in der Palliative Care in der Schweiz
Anne Christine Dölling-Perroulaz, Düdingen CH
Abstract
Hintergrund
Die Lebensende-Doula ist ein neuartiges, auf die Bedürfnisse von schwerkranken Menschen und deren Angehörigen abgestimmtes Unterstützungsangebot, das in der Schweiz zunehmend an Bedeutung gewinnt. Der Begriff "Doula" stammt aus dem Griechischen und bezeichnet ursprünglich eine Begleiterin während Schwangerschaft und Geburt. Nach diesem Modell entstand die Lebensende-Doula, um Menschen in der letzten Lebensphase ganzheitlich zu begleiten. Der Bedarf an einer derartigen Rolle wurde vom Schweizer Bundesamt für Gesundheit (BAG) bereits 2020 in einem Bericht hervorgehoben, insbesondere für Zielgruppen wie Alleinstehende oder Familien mit kleinen Kindern. Ziel Die Lebensende-Doula übernimmt eine komplementäre Rolle im bestehenden Palliativnetzwerk. Sie bietet keine medizinischen Leistungen, sondern konzentriert sich auf psychosoziale, spirituelle, emotionale und praktische Unterstützung, ähnlich einer vertrauten Bezugsperson. Ziel ist es, die Lebensqualität am Lebensende zu verbessern, die Selbstbestimmung zu stärken und Angehörige zu entlasten. Methode Kernaufgaben:
Resultate Die Unterstützung einer Lebensende-Doula kann eine Ergänzung in der Palliativversorgung anbieten, indem sie ein individuelles, nicht-medizinisches Angebot schafft, das Menschen in ihrer letzten Lebensphase umfassend begleitet. Die im März 2026 startende deutschsprachige Ausbildung in Freiburg trägt dazu bei, diese innovative Rolle in der Deutschschweiz weiter zu etablieren. In der Romandie hat das Centre de formation Rosette Poletti, bereits den 10. Ausbildungsvorgang angefangen. Um die 80 Lebensende-Doula sind aktuell aktiv in der Westschweiz. Schlussfolgerung Die Lebensende-Doula ist eine wertvolle Ergänzung in der Palliativversorgung, die auch den Menschen in den Mittelpunkt stellt sowie Angehörige in einer herausfordernden Lebensphase entlastet. Die Integration dieses Berufs in die interdisziplinäre Palliativversorgung bietet Potenzial zur Verbesserung der Lebensqualität am Lebensende und zur Stärkung der psychosozialen Betreuung in der Schweiz der Kranken Person sowie ihrer Angehörigen. |
||
|
P23
Requests for assisted suicide in patients hospitalized in the Geneva University Hospitals, an update.
Monica Escher, Genève CH
Abstract
Contexte
In 2022, the Geneva University Hospitals decided to facilitate the access to assisted suicide (AS) in the hospital to inpatients. A Reference Group for Assisted Suicide (RG) was created whose tasks are 1) support the health care team who are assessing a patient’s request, and 2) meet the health care team in order to ascertain the thoroughness of the assessment process (“validation-no validation meeting”) when they come to the conclusion that the patient should be allowed to commit AS in hospital. Objectiv To determine the characteristics and outcomes of hospitalized patients requesting AS, and the integration of the RG in the assessment process of the requests. Méthode Retrospective review of the electronic medical records of the patients reported to the RG and prospectively collected data related to the activity of the RG. Résultats From July 2022 till April 2025, 69 patients made a request for AS, 20 in 2022, 37 in 2023, 7 in 2024, and 5 in 2025. Mean age was 80.3 years (min 53, max 97), 41 patients were male (59.4%). Cancer was the most common diagnosis (n=33, 47.8%). Half the patients (n=33) were members of a right-to-die association before the index hospital stay. Among patients, 52.2% (n=36) were staying in the acute care hospital, 26.1% in a palliative care unit, and 14.5% in geriatrics. Outcomes were: 17 AS in hospital, 14 AS out of hospital, 22 natural deaths, and 11 patients did not persist in their request. Among the patients committing AS out of hospital, half (n=7) went home and half were transferred to a private medical facility. Nearly half the patients (n=33) were reported to the RG by the palliative care team (n=23, 69.7%) or the psychiatrist. The RG was never contacted by the medical team for 18 of them (54.5%). Reasons for contacting the RG were 1) organization of a validation-no validation meeting (n=34/51, 66.7%), 2) need for information (n=12, 23.5%), 3) reporting of a patient’s request (n=9, 17.6%), and 4) need for support (n=5, 9.8%). Mean number of days between the request for a validation-no validation meeting and the meeting was 7.4 (min 1, max 30), and the median was 5 days. Non validation occurred in 3 cases (8.8%). Mean number of days between the meeting and AS in hospital was 7.3 (min 1, max 27), and the median was 6 days. Mean number of hospital days before the AS in hospital was 51.5 (min 21, max 188), and the median was 39 days. Conclusion The characteristics and outcomes of inpatients requesting AS are varied, but palliative care units are particularly exposed to those requests. The Reference Group is mostly integrated at the end of the assessment process and seldom asked for support. 
|
||
|
P24
Projekt ‘Care for the Carers’: Selbstfürsorge und Resilienz von Gesundheitsfachpersonen stärken
Sibylle Felber, Bern CH
Abstract
Hintergrund
Fachpersonen im Gesundheitswesen stehen durch steigende berufliche Anforderungen durch die zunehmende Komplexität der Patient:innen (Multimorbidität, Hochaltrigkeit etc.), personelle und ökonomische Ressourcenknappheit sowie dauerhafte emotionale Belastung und komplexere Administration unter hoher Belastung. Gleichzeitig wird von ihnen erwartet, professionell und mitmenschlich für andere zu sorgen, selbst gesund zu bleiben und sich sowohl fachlich als auch persönlich kontinuierlich weiterzuentwickeln. Ziel Das Projekt will Fachpersonen im Gesundheitswesen darin bestärken, sich selbst Sorge zu tragen und so eine verlässliche Grundlage zu haben, um für andere Menschen hilfreich zu sein. Methode Aufgrund einer Bedürfnisanalyse von Fachpersonen, die chronisch und schwer erkrankte Menschen begleiten, wird ein innovatives, evidenzbasiertes Bildungsangebot zur Förderung von Selbstfürsorge und Resilienz entwickelt. Elemente wie Selbstmitgefühl, Achtsamkeit und Selbstreflexion sollen gestärkt werden und dabei unterstützen, persönliche Ressourcen zu aktivieren und Herausforderungen des Berufsalltags empathisch zu begegnen. Kernstücke des modularen Bildungsangebotes sind individuell nutzbare Lernprogramme sowie ein niederschwelliger Workshop, welcher inhouse von bereits vor Ort angestellten, kompetenten ‘Facilitators’ oder bei Bedarf durch externe Fachpersonen durchgeführt werden kann. Resultate Die entwickelten Module sollen übertragbar auf andere Fachbereiche und Institutionen sein, wodurch die Anfangsinvestitionen nachhaltig wirken. Die Online-Bereitstellung ermöglicht eine breite Dissemination und einfache Integration in den Berufsalltag sowie bereits in der Ausbildung. Der Facilitator-Leitfaden sichert die langfristige eigenständige Umsetzung der Massnahmen. Eine feste Integration in Weiterbildungsprogramme wird angestrebt. Schlussfolgerung Das Projekt verfolgt einen ganzheitlichen Ansatz, der persönliches Wohlbefinden und ‘Selbstsorge’ mit beruflicher Professionalität verbindet, gemäss dem Leitsatz «Für andere da sein, ohne sich selbst zu verlieren». Das innovative Bildungsangebot hat das Potenzial, nicht nur die Gesundheit und Resilienz von Fachpersonen zu stärken, sondern auch die Qualität der Patientenversorgung zu verbessern, da empathische und resiliente Fachpersonen ihre Kompetenzen optimal einsetzen können. |
||
|
P25
Transsektorieller Personalaustausch für Anbieter der spezialisierten Palliative Care – ja, aber wie?
Monica Fliedner, Bern CH
Abstract
Hintergrund
Wegen komplexen Situationen wechseln PatientInnen im Krankheitskontinuum der (spezialisierten) Palliative Care immer wieder zwischen den Sektoren Spital – Zuhause – Pflegeeinrichtungen. Um die Fragmentierung im Gesundheitswesen zu überbrücken, und um chronisch kranke Menschen entsprechend ihren Bedürfnissen zu versorgen, werden innovative Modelle diskutiert. Ein Personalaustausch zwischen den Sektoren kann für Pflegende bereichernd und motivierend sein, im Fachgebiet zu bleiben. Dabei sind Kollegialität, Interprofessionalität, und Zweckmässigkeit massgebend. Ziel Ziel war, die inter- und intraprofessionelle Zusammenarbeit zu verbessern, die Patientensicherheit zu erhöhen, Schnittstellen zu optimieren und die Rolle der spezialisierten Pflegenden zu stärken. Methode Ein Konzept mit Kooperationsvertrag wurde zwischen vier Anbietern der stationären und ambulanten spezialisierten Palliative Care verabschiedet. Auf Grund einer Literatur- und SWOT-Analyse wurden Bedingungen für eine Pilotphase mit Personalaustausch definiert:
Vor Start und am Ende des Pilots wurde ein Fragebogen zur Evaluation der negativen und positiven Erwartungen bzw. Erfahrungen an die MitarbeiterInnen der teilnehmenden Institutionen geschickt. Resultate Zwei Pflegende nahmen für 6 Monate zu je 20% am Personalaustausch zwischen mobilem Palliativdienst und Palliative Care Konsildienst teil. Der Wissenszuwachs, die Erfahrungen und die Zusammenarbeit zwischen den Sektoren wurden gestärkt, Schnittstellen zu Gunsten einer idealen Versorgung der PatientInnen wurden optimiert, und die professionelle Entwicklung der MitarbeiterInnen wurde unterstützt. Es wurde wahrgenommen, dass 20% für den Personalaustausch zu wenig sind, um ein besseres Verständnis für Bedürfnisse und Arbeitsweisen im anderen Sektor zu erhalten. Der Einführungsbedarf bei fehlenden Vorkenntnissen der Institution war hoch, aber die Zusammenarbeit und das gegenseitige Verständnis wurden gefördert, wobei unterschiedliche Prozesse und Dokumentationssysteme (digitale KG) herausfordernd waren. Schlussfolgerung Verbesserung der Schnittstellen und damit eine höhere Versorgungsqualität wurde erreicht. Einige Korrekturen (z.B. Personalaustausch mit höher-prozentigen Mitarbeiterinnen) wurden umgesetzt. Eine zweite Pilotphase, die ebenfalls vergleichbar evaluiert wird, läuft bis September 2025. Resultate werden vorliegen. |
||
|
P26
Spiritual Needs in Palliative Care Inpatients: Five Years of Clinical Data of a Swiss Tertiary Care Center
Valentin Frei, Zurich CH
Abstract
Hintergrund
Spiritual and religious needs are increasingly recognized as essential components of holistic palliative care. However, structured assessment and documentation of these needs remain inconsistent in clinical practice. Ziel This study aims to identify and categorize spiritual needs among patients in a tertiary palliative care setting. Methode A retrospective, single-center study was conducted at the Acute Palliative Care Unit (APCU) of the University Hospital of Zurich. Electronic health records (EHRs) of 1049 patients admitted between 2019 and 2022 were screened. Of these, 747 records with encodable spiritual or psychological content were included. Qualitative content analysis was used to identify recurring themes in documentation by pastoral and psychological services. Needs were categorized using a framework adapted from Selman et al. Resultate A total of 22 distinct spiritual needs were identified and grouped into four main domains: existential, psychological, social/relational, and religious. Psychological services documented spiritual needs in 85.4% of cases, while pastoral care did so in 49.2%. The most frequently recorded needs included existential fears, biographical reflection, and relational concerns. Religious needs were less commonly documented, with notable variance between care providers. Schlussfolgerung This is the first study in Switzerland to systematically examine the spiritual needs of palliative patients through clinical documentation. Findings highlight the significance of spiritual needs at the end of life and underscore the lack of standardized communication and documentation practices. Improved tools and interprofessional strategies are necessary to better identify and address spiritual concerns in palliative care settings. |
||
|
P27
Dexmédétomidine facilitant la guérison d’un trouble de l’humeur chronique menant à une maturation.
Dr Wilhelm Freiherr von Hornstein, Cullies, Co. Cavan IE
Abstract
Contexte
Une femme de 77 ans souffrant d’un trouble de l’humeur chronique, suivie en psychiatrie depuis 40 ans, fut hospitalisée deux fois une année entière en psychiatrie après immolation suicidaire et mort dramatique par cancer de deux de ses filles, sexuellement abusées comme enfants. Après hospitalisation pour une maladie pulmonaire obstructive chronique (MPOC) avec insuffisance respiratoire de type II, le service des soins palliatifs fut consulté lorsqu’elle devint plus anxieuse et tolérant moins bien le masque à pression positive continue des voies respiratoires (PPC). Comorbidités furent : Diabète de type II, hypothyroïdie, cachexie. Objectiv Réflexion sur l’usage bénéfique de la dexmédétomidine, un agoniste des récepteurs alpha2-adrénergiques avec des propriétés anxiolytiques, comme alternative pour une patiente souffrant d’un trouble de l’humeur chronique résistant aux traitements médicamenteux et électro-convulsifs psychiatriques. Méthode Démographie, histoire médicale, traitements, effets secondaires, et paramètres cardio-vasculaires furent relevés. Résultats Malgré une médication psychiatrique journalière de duloxétine 120 mg, pregabalin 100 mg, Na-valproate 600 mg, olanzapine 7,5 mg, alprazolam 0,5 mg et témazépam 10 mg elle continuât à être très anxieuse et commençât d’avoir des difficultés à prendre tous ces médicaments par voie orale. La dexmédétomidine fut introduite comme perfusion sous-cutanée continue pour une période de 47 jours. Avec une dose de 0,24 µg/kg/h elle se stabilisa et fut transférée après 2 semaines d’une unité de soins aigus à une unité de soins de fin de vie. Après 30 jours elle commença à développer des périodes d’hypotension artérielle nécessitant une réduction de la dose de dexmédétomidine pour l’arrêter complètement après 17 jours. Elle continuât pour soulager la détresse respiratoire avec une perfusion sous-cutanée continue d’alfentanil IC 15 mg et halopéridol 3,5 mg / jour. À partir de cette période son niveau d’anxiété commença à baisser tout en demeurant très en colère. Elle fut plus ouverte à des conversations et acceptât, puisqu’elle continuât à survivre, d’être transférée dans un établissement médico-social. Puis arriva la crise transformatrice. « Elle voit la présence de ses deux filles décédées » ce qui la troubla profondément mais lui permît de surmonter son anxiété et sa colère. Elle décida de rentrer à la maison et créer des liens avec ses petits-enfants. Conclusion En soulageant ses symptômes physiques sans sédation profonde elle accéda sa profondeur tout en utilisant sa résilience pour une maturation inespérée. |
||
|
P28
Improved Management of Seizures with Brivaracetam Continuous Subcutaneous infusion (CSCI)
Dr Wilhelm Freiherr von Hornstein, Cullies, Co. Cavan IE
AbstractContexte The anti-epileptic Brivaracetam, licensed in 2016, is associated with fewer behavioural or psychiatric side effects than levetiracetam. The maximal dose can be accommodated in a single syringe driver. When oral intake becomes problematic Brivaracetam can be converted 1:1 to a continuous subcutaneous infusion (CSCI). Objectiv To improve seizure management in a palliative care setting. Méthode 25 Patients referred to a Specialist Palliative Care Service showing seizure activity were analysed. Noted: - Demographic data - Diagnosis - Symptoms - Medications - Indications for anti-convulsive treatments - Results - Outcome Résultats Patients: mean age 72 years, 16 male, 9 female. Treated were seizure activity originating from malignant (9) and non-malignant (16) underlying diseases. 8 patients pretreated with levetiracetam were switched to brivaracetam at a ratio of 10:1. They all showed reduced seizure activity, became more alert and were emotionally more stable. Some patients dying in an unconscious state regained some consciousness which allowed them to interact with their families. 4 patients needed a second (lacosamide, midazolam, phenobarbital or Na-valproate) and three patients a combination of 3 anti-epileptics. One ventilated patient with excessive bronchial secretions (vegetative seizure activity) could be weaned off and moved to a ward after a first failed extubation. While all patients died one lady with a massive intra-cerebral bleed made an unexpected recovery, could be switched to oral medication and was discharged home 5 months later after recovering her swallow, speech and mobility. In total 563 days of CSCI treatment days were documented. Doses ranged from 100 to 200 mg per day, diluent water for injection. The subcutaneous infusion site remained functional up to 7 days, no local skin irritation observed. Conclusion Brivaracetam 1% solution is well tolerated and can safely be administered as a CSCI to manage better seizure activity with less side-effects. |
||
|
P29
Gesundheitliche Vorausplanung in Basel-Stadt - eine multizentrische Befragungsstudie
Katharina Froelich, Basel CH
Abstract
Hintergrund
Gesundheitliche Vorausplanung (GVP) bezeichnet den Prozess, durch den Patient*innen ihre zukünftige Gesundheitsversorgung im Voraus planen, insbesondere im Hinblick auf Entscheidungen am Lebensende oder bei schwerer Krankheit. Trotz eines allgemeinen Bewusstseins für die Bedeutung von GVP steht eine systematische Integration in bestehende klinische Behandlungspfade noch aus. Ziel Ziel der Studie ist es, die aktuelle Anwendung von GVP in verschiedenen Institutionen und Sektoren der Gesundheitsversorgung des Kantons Basel-Stadt zu untersuchen. Aus den Ergebnissen der Standortbestimmung sollen Strategien für die Implementierung regional entwickelter Formulare der GVP abgeleitet werden. Methode Von Oktober bis Dezember 2024 wurden Gesundheitsfachpersonen mittels Convenience-Sampling rekrutiert, die in unterschiedlichen Institutionen der gesundheitlichen Versorgung (Universitätsspital, Hausärztliche Praxen, Alters- und Pflegeheime, spezialisierte Palliative Care) des Kantons Basel-Stadt tätig sind. Die Befragung mit 35 Ratingfragen und sechs offenen Fragen wurde je nach Zielgruppe online oder auf Papier durchgeführt. Hierbei wurden die Anwendung spezifischer Formulare (Patientenverfügung, Ärztliche Notfallanordnung, Behandlungsplan), Einstellungen gegenüber GVP sowie Barrieren und unterstützende Massnahmen bei der Integration von GVP untersucht. Resultate Insgesamt nahmen 212 Gesundheitsfachpersonen aus den verschiedenen Sektoren mit überwiegend langjähriger professioneller Erfahrung an der Studie teil. Spezifische Formulare der GVP sind bekannt und werden im geringen Umfang bereits angewandt. Generell gibt es positive Einstellungen gegenüber GVP. Hauptsächliche Barrieren sind fehlende personelle Ressourcen sowie die lange Dauer der Beratungsgespräche. Verschiedene Massnahmen wurden von den Teilnehmenden als unterstützend bei der Anwendung von GVP eingeschätzt. Schlussfolgerung Die Studie trägt dazu bei, ein besseres Verständnis der aktuellen Anwendung von GVP im Kanton Basel-Stadt zu entwickeln und durch die Identifikation von Barrieren und Unterstützungsmassnahmen konkrete Empfehlungen für eine effektive Implementierung der kantonalen GVP-Dokumente zu formulieren. |
||
|
P30
PALLIATIVE CARE AND DISABILITY: WORKING IN PROGRESS
Tanja Fusi-Schmidhauser, Lugano CH
Abstract
Contexte
The estimation about the global prevalence of people living with intellectual disability is approximately between 1% and15%. The life expectancy for adults with developmental disabilities increased in the last decades. During their disease trajectory, they experience complex and multidimensional palliative care (PC) needs that are seldom met by specialized PC teams. This lack of equitable access to PC services might reduce quality of life of patients with developmental disabilities and their informal careers. Objectiv To illustrate the challenges of caring for patients with developmental disabilities in a specialized PC unit. Méthode Clinical study in a specialized PC unit. A 26-year-old patient with an ATR-X genetic syndrome was transferred to our unit after being hospitalized for five months in intensive care, where he underwent eight surgeries and several cycles of antibiotic therapy for toxic megacolon with perforation. ATR-X is a congenital condition characterized by mild to severe intellectual disability, facial, skeletal, urogenital and hematopoietic anomalies. Furthermore, gastrointestinal complications, seizures, visual and auditory impairment are often associated. The specialized PC team was called on consultation for discussions about advance care planning with the parents, after the intensive care unit team excluded further invasive treatment for arising complications. Résultats During one month of hospital stay in our unit, several challenges were encountered while caring for this patient. Unaccustomed healthcare professionals to patients with developmental disabilities, longstanding disease trajectory with unrealistic “hope” expressed by the family and clinical complexity as a barrier to home discharge and the need for relocation were amongst the main issues observed during hospital stay. Conclusion Patients with developmental disabilities with PC needs must benefit from early PC interventions to improve their quality of life. Symptom management, discussions about advance care planning and preferred place of care are essential in this longstanding disease trajectory. Healthcare professionals’ education and novel policies in the healthcare system are deemed necessary to promote equitable access to high-quality PC. |
||
|
P31
Caring for Palliative Carers: Exploring Virtual reality for Professional Well-being
Tanja Fusi-Schmidhauser, Lugano CH
Abstract
Contexte
Interprofessional teams working in specialist palliative care (PC) units are confronted with different degree of emotional and psychological stress. Virtual reality (VR) interventions are described in recent literature as being safe and effective for symptom control for PC patients, especially for pain management. Furthermore, VR was used for healthcare professionals (HCP) in various care settings to reduce subjective stress, but data in specialized PC units are scarce. Objectiv To explore the experience of VR and its impact on well-being for HCP working in specialized PC units. Méthode Explorative pilot study conducted from August 15 to September 15, 2024 in two specialized PC units. Demographics and data on VR experience were collected through a duly developed questionnaire. HCP completed the questionnaire after a 10-minutes VR session. Descriptive statistics supported data analysis. Résultats Twenty-one HCP (18 nurses, 2 physicians, 1 allied HCP) participated in the study. A total of 76% of all participants (n=16) had never experienced a VR session and 90% (n=19) concluded the 10 minutes session. Perceptions of relaxation was described by 80% (n=17) of all participants, 29% (n=6) recounted a leisure-like moment and 24% (n=5) reported a sensation of well-being. Minimal side-effects such as nausea and dizziness were mentioned by 42% (n=9) of all participants, but only 10% (n=2) interrupted the session. Furthermore, 86% (n=18) stated that VR might be useful for improving HCP well-being in specialized PC units, especially after a stressful event. Conclusion The routine implementation of VR sessions for HCP might represent an effective support to improve perceived well-being, particularly after stressful episodes and as a valid alternative to scheduled work breaks. Further studies in our institution are planned to confirm the results of this exploratory pilot study. |
||
|
P32
Posttraumatic growth in palliative care: Exploration of patients’ experiences through life narrative
Laura Galbiati, Lausanne CH
Abstract
Contexte
Posttraumatic growth (PTG) refers to positive psychological changes occurring after an adverse life event. Most research is based on transversal research designs in cancer using the Post-Traumatic Growth Inventory (PTGI). Studies do not provide an understanding of how this process may develop, especially regarding the patient's life trajectory. Objectiv Through life narrative interviews, our study aims (i) to describe profiles of psychological changes experienced by palliative care patients, and (ii) to link these profiles with quality of life and PTGI. Méthode This study adopted a multi method design. Semi-structured interviews based on the Biographic Narrative Interpretive Method were conducted in three palliative care centres in Switzerland. An ideal-type analysis was used to establish profiles of patients and a thematic analysis to characterize these profiles. In addition, the PTGI and the McGill Quality of Life-Revised questionnaire (MQOL-R) were used. Résultats A total of 23 patients participated (13 female, median age = 73, 13 with cancer). The ideal-type analysis revealed four profiles of changes: (i) “Overcoming adversity” (n=6), characterized by positive psychological changes, future plans, strong social support, and medical staff satisfaction; (ii) “Resilience” (n=7), characterized by less positive psychological changes but effective daily coping strategies; (iii) “Resignation” (n=3), marked by illness acceptance and serenity toward death; and (iv) “Psychological suffering” (n=7), characterized by severe distress, despair, and end-of-life preparation. The profiles “Overcoming adversity” and “Resilience” showed higher PTGI scores than “Resignation” and “Psychological suffering”. MQOL-R scores were more homogeneous between the groups. Conclusion Life stories offer an innovative way to understand changes during serious illness and end-of-life. The variability of the profiles shows the value of considering the patient beyond end-of-life issues. Patients’ reactions to illness may be strongly conditioned by their life trajectory. We encourage professionals to use narrative approaches integrating the patient’s life story into their clinical practice.
|
||
|
P33
How to Say Goodbye? Strategies for difficulties in interview closure with end-of-life patients
Laura Galbiati, Lausanne CH
Abstract
Contexte
Vulnerability is a central concern in human research fields such as sociology, psychology, nursing, and ethics. However, this concept has been often addressed through the researcher’s effort to minimize risks and prevent potential negative consequences for participants throughout the study, particularly when conducting an interview. When doing research in palliative care, this question is essential, because researchers are generally confronted with vulnerable patients. In addition to the palliative medical issues, symptoms such as social distress, anxiety, fatigue may arise during the interview. Conducting research in the context of the end-of-life care potentially exposes researchers to several challenges. These can be especially present during interviews, which might confront them with their own vulnerabilities. This confrontation can be challenging and could affect their own well-being. Objectiv We aim to share and compare our field experiences as researchers and the challenges faced when meeting and leaving vulnerable patients and illustrate our experiences through two different vignettes. Méthode Our research team consists of early-career female researchers working in the palliative and supportive care service. During collective reflexivity workshops, we share our field experiences and provide feedbacks to improve our role and our research practices when meeting participants. Common challenges and themes that emerged from the discussion were extracted, condensed and illustrated through vignettes. Résultats The vignettes are drawn from our field experiences and offer reflections and practical insights to enhance our roles and research practices during participant encounters. By comparing our experiences of interviewing patients at the end of life, we identified the concluding phase of the interviews as a common challenge. One of the most delicate aspects we faced was how to say goodbye to patients we had come to know personally through the interviews—individuals who were likely to pass away in the near future. Conclusion Based on the field experiences of researchers, two different vignettes highlight challenges in interview closure with end-of-life patients. The common difficulties reveal the challenges related to researchers’ interpersonal skills in palliative care, and the need to create spaces such as workshops where they can express themselves, share experiences, and find guidance. |
||
|
P34
Tailoring Respectful & Understanding SupporT for LGBTIQ+ people in Palliative & End-of-Life Contexts
Claudia Gamondi, Lausanne CH
Abstract
Contexte
Lesbian, gay, bisexual, trans, intersex, queer/questioning (LGBTIQ+) individuals experience challenges in accessing inclusive healthcare. These challenges stem from systemic discrimination, cultural misunderstandings, and structural barriers within healthcare systems, which lead to mistrust and reluctance to seek care. Social isolation, reliance on “families of choice,” and lack of healthcare provider (HCP) awareness complicate palliative and end-of-life care (PEOLC) experiences. In Switzerland, the unique needs of the LGBTIQ+ population are poorly understood and insufficiently addressed in PEOLC policies and practices. Objectiv This represents a study protocol of research investigating the needs, challenges, and preferences of LGBTIQ+ individuals and their chosen families in PEOLC in Switzerland. It also aims to examine HCPs’ understanding and practices concerning inclusive care. Méthode We will employ a Participatory Action Research (PAR) approach, which emphasizes collaboration with LGBTIQ+ associations, HCPs, and key stakeholders to co-create knowledge during the project’s planning, data collection, analysis and dissemination phases. This method ensures that we do not merely observe but actively engage participants in the research. A scoping review of existing scientific and grey literature will map current knowledge and identify gaps. Research methods also include secondary data analysis and qualitative/quantitative data collection methods with LGBTIQ+ individuals, their chosen families, and HCPs from Switzerland’s 3 main linguistic regions. Résultats Anticipated benefits include developing inclusive care practices, enhancing trust in healthcare systems, and reducing health disparities. An important project outcome is the co-creation of a Rainbow Book, a resource including practical recommendations for HCPs and policy recommendations promoting more equitable PEOLC. Conclusion Project outputs will provide a foundation for systemic change in the healthcare system, ensuring that LGBTIQ+ individuals receive respectful care in their final stages of life. By engaging communities directly through PAR, the project seeks not only to generate new insights but also to foster lasting trust in PEOLC practices and policies across Switzerland. |
||
|
P35
Healthy dying: promoting health until death?
Josepha Girard, Fribourg CH
Abstract
Contexte
‘We all die, but how do we die? That is the question’. A 2 ECTS elective module has been developed for 3rd year students at the Heds FR to attempt to answer this. Empowerment is a central concept for this theme, reflecting changing societal attitudes (Catford, 2018). Palliative care is centred on compassion, dignity and gratitude, while the concept of ‘healthy dying’ is more recent. Nurses play a key role in transforming community perceptions of the end of life through their role in coordinating care (Abel et al., 2018). Objectiv The objectives of the module were as follows:
Méthode In groups, the students analysed a clinical vignette of a person being cared for in different care settings. Concurrently, the students expanded their theoretical understanding of the various themes and concepts surrounding 'dying in health'. The analysis was based on the problem tree method, a technique that facilitates the identification of the causal links between the various factors that underpin the problem (Chaput, 2021; Gircourt, 2020). This method involves the creation of two trees: a problem tree and a solution tree. For the purposes of this module, the latter has been termed the 'person's life project tree'. Résultats When evaluating the module, students offered a number of constructive comments and suggestions. The feedback indicated a need for more practice and originality. We have therefore decided to enhance the module for the next intake in 2026 by incorporating simulations, site visits and a testimonial. Students will have the opportunity to test their solution tree and practise announcing a death using simulations. Conclusion The optional module provided students with an opportunity to reflect on the following questions: ‘Is it possible to promote health right up to the end of life? ‘What are the limits? |
||
|
P36
Pädiatrische Palliative Care für Kinder mit komplexen oder fortgeschrittenen Herzerkrankungen
Deborah Gubler, Zürich CH
Abstract
Hintergrund
Kinder und Jugendliche mit progredient verlaufenden Erkrankungen oder komplex chronischen Krankheitsbildern, die nicht oder nicht mehr von einer kurativen Behandlung profitieren, oder bei denen eine hohe Unsicherheit in Bezug auf die Behandelbarkeit der Erkrankung besteht, leiden häufig unter einer Vielzahl komplexer medizinisch-pflegerischer, seelischer und/oder sozialer Probleme, die sich auf die gesamte Familie und das Umfeld auswirken. Die Fortschritte in der pränatalen Medizin führen manchmal zur (Verdachts-) Diagnose einer Erkrankung ohne Heilungsaussicht und zum Bedarf einer palliativen Begleitung. In diesen Situationen kann ein Involvieren des interprofessionellen Pädiatrischen Palliative Care (PPC) Teams sinnvoll sein. Palliative Behandlungs- und Betreuungskonzepte haben zum Ziel, jede Lebensphase eines Kindes im Umfeld der Familie mit einem hohen Grad an Selbstbestimmung bestmöglich zu gestalten. Der Einbezug von PPC am Universitäts-Kinderspital Zürich war noch nicht standardisiert und hatte entsprechend (zu) späte Zuweisungen zur Folge. Nicht zuletzt war einer der Gründe, dass die Leistungen des PPC Teams den Teams des Kinder-Herzzentrums nicht umfassend bekannt waren. Ziel Etablieren von Standards einer palliativen Betreuung, zu der jedes Kind von 0-18 Jahren mit komplexer oder fortgeschrittener Herzerkrankung und deren Familie Zugang haben soll. Damit verbunden eine Optimierung der Zusammenarbeit und Abläufe der interprofessionellen Teams Kinder-Herzzentrum und PPC. Methode Im ersten Schritt Bildung einer interprofessionellen Arbeitsgruppe mit Vertretung aller Kerndisziplinen des Kinder-Herzzentrums und PPC, welche gemeinsam anhand von internen Erfahrungen, internationalen Empfehlungen und eigenen sowie internationalen Forschungsergebnissen die Kernthemen für Standards und die Optimierung der Zusammenarbeit definieren und ausarbeiten. Im zweiten Schritt Validierung der Umsetzung mittels Fragebogenbefragung und Fokusgruppe. Resultate Das Konzept «Pädiatrische Palliative Care – Konzept für Kinder mit komplexen oder fortgeschrittenen Herzerkrankungen» hat als Kernstück gemeinsam erarbeitete Indikationskriterien für eine Zuweisung ans PPC Team. Dies ist ein Novum und hat zu einer niederschwelligeren Zuweisung und Verdopplung der Patient:innen mit kardiologischen Diagnosen in der PPC geführt. Das Konzept wird seit 2024 umgesetzt. Aktuell läuft eine Validierung intern. Schlussfolgerung Ein spezifisches PPC Konzept für die Population Kinder mit Herzerkrankungen kann sich positiv für die Betreuung der betroffenen Kinder und die interdisziplinäre Zusammenarbeit auswirken. Eine Übertragbarkeit auf andere Disziplinen und/oder Zentren kann geprüft werden. Die Resultate der Fragebogenbefragung werden präsentiert. |
||
|
P37
Abendländische Spiritualität als Ressourcen für betreuende und pflegende Angehörige
Loretta Hasler, Maienfeld CH
Abstract
Hintergrund
Betreuende und pflegende Angehörige werden häufig konfrontiert mit ihren Grenzen der Hilfemöglichkeiten gegenüber der zu betreuenden Person sowie auch mit der Reduktion ihrer eigenen Kräfte. Man sucht nach Unterstützungsmöglichkeiten für sich und der hilfebedürftigen Person. Ziel Mit der Frage nach dem Sinn des Lebens wird häufig auch das Bewusstwerden des endlichen DASEINS entdeckt. In unserer abendländischen Kultur wurde uns das Instrument zu Verbindungen von geistlichen spirituellen Ebenen geschenkt. Es gilt aus diesem historischen Hintergrund sowie aus den Erfahrungen des Alltags diese Kräfte wieder wahrnehmen zu können. Methode Interssierten Angehörigen werden Impulse der spirituellen Quellen mittels Wort, Bild und Musik mittels Seminarangeboten übermittelt. Resultate Die Seminarangebote bestehen immer noch. Jede einzelne Person nimmt für sich das für sie eigene wertvolle Ergebnis mit in ihren Alltag. Es ist nicht geplant, dass "qualitiy of life" Fragebogen nach den Seminaren aufzuzeichnen sind. Diskussion Geht man der Frage des Sinns des Lebens nach, so wird man mit dem Sterben und der Endlichkeit unseres jetzigen Daseins konfronitert. Die materiellen Gegenstände bekommen weniger Bedeutung. Man sucht nach weiteren Ressourcen, die ausserhalb des eigenen Ichs entdeckt werden können. Wie AHA Erlebnisse beim Erstaunen eines Bildes, beim Hören einer Musik, beim Bewundern der Natur, beim ersten Lächeln eines Kindes und so weiter. Diese aufkommende Gefühle sind ureigene Gefühle, die plötzlich da sind. Woher kommen diese? Welche Verbindungen haben wir mit dem All? Wo kann ich diese Ressourcen bei den alltäglichen Aufgaben einsetzen? Schlussfolgerung Immer mehr wird unserer Gesellschaft bewusst, dass wir Teil in einem Kreislauf des Universums sind mit Werden, Sein und Vergehen. Mit den Gedanken der Spiritualität kommen wir in Berührung der Unendlichkeit. Das kann uns Türen öffnen zur Ehrfurcht gegenüber etwas Grösserem als wir sind und zur Demut. Es bietet auch eine Möglichkeit, indem wir über uns hinauswachsen können. Wir finden in uns mehr Ruhe und weniger Angst. |
||
|
P38
Seizures in end-of-life care in primary and in secondary brain tumors
Zehra Hepp, Winterthur CH
Abstract
Hintergrund
Epileptic seizures are a frequent complication in patients with primary or secondary brain tumors and can significantly impact their quality of life. These seizures may arise at different stages of the disease — early on, as the disease advances, or during the end-of-life (EOL) phase. However, research addressing the frequency and management of seizures in palliative care patients remains limited. Ziel The aim of this study was to examine the prevalence and characteristics of seizures during the last month before death in patients with primary or secondary brain tumors treated in a tertiary palliative care unit. Methode In this retrospective cohort study, we analyzed patients with primary or secondary brain tumors who died at the palliative care competence center at the University Hospital of Zurich (2018–2024). Analyzed data included demographics, disease characteristics, prior treatments, and occurrence of seizures. EOL phase was defined as the last month before death. Statistical analyses examined associations between clinical characteristics and occurrence of EOL seizures. Resultate A total of 143 patients was included, 14.7% (n=21) of these suffered from EOL seizures. Patients with primary brain tumors were more likely to experience seizures (32.4%, n=11) than patients with secondary brain tumors (9.2%, n=10; p<0.001). A prior history of epilepsy was associated with an increased seizure risk in EOL; 31.7% (n=13) of patients with prior epilepsy suffered from EOL seizures vs. 7.8% (n= 8) patients without prior diagnosis (p<0.001). Despite being under antiepileptic therapy, 47.6% (n=10) of patients with EOL seizure experienced recurrent seizures during EOL. The most commonly prescribed antiepileptic medication was levetiracetam (30.1%, n=43). Schlussfolgerung Primary brain tumors and prior history of epilepsy were strongly associated with occurrence of EOL seizures. Effective seizure management is essential in palliative care.
|
||
|
P39
Symptom burden, place of death, and implications for end-of-life care in glioma patients
Caroline Hertler, Zürich CH
Abstract
Hintergrund
Patients with primary brain tumors suffer from a high symptom burden combining neurological and oncological symptoms, with physical and neurocognitive deterioration already at early stages of the disease. Moreover, high grade gliomas have a very poor survival rate, leaving very little time to prepare for palliative and end-of-life related situations. Ziel Here, we aim at characterizing the relationship between symptom burden, advanced care planning and place of death in patients with glioma. Methode In this retrospective study, we analyzed 394 patients with glioma treated at the Comprehensive Cancer Center Zurich between 2015 and 2023. We investigated demographics including last place of care, clinical information, symptom burden and characteristics of advanced care planning and palliative care. Statistical analysis was performed to determine associations between variables. Resultate Most patients included suffered from a WHO grade 4 gliomas (88%, n=347). Patients had a median age of 60 years (IQR 50-69) at diagnosis, and a median age of 62 years (IQR 52-70) at death. Median overall survival was 1.49 years (IQR 0.97-2.46). Patients suffered from high symptom burden in the last phase of life, including motor dysfunction (66%, n=261), neurocognitive decline (48%, n=155), and speech impairment (39%, n=155). Seizures occurred in 20% (n=77). Almost half of patients suffered from more than 3 symptoms (46%, n=180). Of patients with know place of death, 32% (n=58) died in inpatient palliative care, 26% (n=46) at home, and 16% (n=28) each in either hospice care or institutions. Higher symptom burden and higher WHO grade were independently associated with inpatient death (p<0.05). A total of 67.5% (n=185) patients were referred to specialist palliative care. However, advanced directives were rarely documented or lacking. Schlussfolgerung Due to early neurocognitive deterioration and high symptom load, patients with gliomas qualify well for early integration of palliative care support and advanced care planning. Identifying patients’ preferences for treatment and last place of care would allow for better patient care in the last period of life. |
||
|
P40
Sterbende als Lehrende im Hospiz: „In meinen Augen danach riefen das man sie im öffentlichen Raum behandelt.“
Anja Herzog, Berlin DE
Abstract
Hintergrund
In vorangegangenen Studien berichteten Sterbende von unangemessenen zwischenmenschlichen Beziehungen zu Gesundheitsakteur:innen oder der fehlenden Beteiligung in Entscheidungsprozessen. Sie dürfen nach wie vor in gesundheitsbezogenen Fragen, bspw. im G-BA nicht mit abstimmen. Ziel Daher widmet sich die Frage dem gesundheitlichen Erleben der Sterbenden in einem nationalen Erwachsenen-Hospiz. Die Frage zielt(e) auf einen reflektierenden Lehr- und Lernprozess ab, in dessen Rahmen Erfahrungen dialogisch ausgetauscht werden. Methode Die wissenschaftstheoretische Basis konstituiert sich aus einem spezifischen Zusammenspiel dreier Elemente (Sozial-Hermeneutik, Lebensweltliche Ethnografie & Reflexiv Grounded Theory), bei dem die Erfahrungen der Teilnehmenden eine zentrale Rolle einnehmen. Als Forscherin erhalte ich über meine eigene Subjektivität Einblicke in die Erfahrungen anderer, wie die der drei Sterbenden, die sich in Expert:innengesprächen in einem stationären Hospiz äußerten. Ergänzt wurde das Datenmaterial durch meine Präkonzepte sowie durch das fortlaufende Führen von etwaigen Memo-Varianten, bspw. dem Leitfaden-Memo oder dem Durchführen eines kulturellen Zirkels in schriftlicher Form. Die Auswertung des Datenmaterials erfolgte in einem drei-schrittigen Kodierprozess, der sich an den Prinzipien der Grounded Theory (offene, axiale & selektive Kodierung) orientiert. Ein Indikatorenschema, was auf den Phasen des hermeneutischen Verstehensprozess basiert, wurde mit hinzugezogen. Resultate Das Ergebnis verdeutlicht die Bedürfnisse nach Harmonie, Zuneigung und Loyalität. Im stationären Hospiz schöpfen sie aus den Ressourcen der Kommunikation. Ein Appell an die Mitmenschen, die gegenwärtigen Rahmenbedingungen zu thematisieren, wird formuliert: "Aus meiner Perspektive wurde das Bedürfnis geäußert, dass sie im öffentlichen Raum behandelt werden." (B III-Z.147- 148[EB1] ), bspw. die Schmerzen, die es bereitet, die eigene Wohnung verlassen zu müssen. Sie berichten auch von ihrem Schutzfaktor, der Liebe, sind sie sich Mitmenschen bewusst, die dafür sorgen, dass es ihnen immer gut gehen wird. Diskussion Zu diskutieren ist einerseits die wissenschaftstheoretische Basis, andererseits damit einhergehend die Art der Datenauswertung. Die Entscheidung für den Drei-Klang resultierte aus der Doppelperspektive der Forscherin. Eine erhob Datenmaterial und setzte diese in Beziehung. Eine weitere speiste sich aus den Handlungsdaten, wie den Interaktionen. Diese Basis versuchte die Reproduktion von kolonialisierenden Diskursen zu vermeiden/ zu verringern. Schlussfolgerung Die Sterbenden im stationären Hospiz sensibilisieren für das Selbstverständliche. Im Hinblick auf zukünftige Entwicklungen ist es selbstverständlich geboten, dass Sterbende in Entscheidungsprozessen, die im G-BA geführt werden, partizipieren. Das Hospiz als Raum ohne physische Grenzen. |
||
|
P41
Komplementäre Behandlungsmethoden in der Palliative Care:Eine qualitative Studie im Bachelor Pflege
Gabriela Hofstetter, Fribourg CH
Abstract
Hintergrund
Komplementäre Behandlungsmethoden wie Phytotherapie oder Anthroposophische Medizin sind in der Schweiz Teil der Grundversicherung. Diese Methoden ergänzen die Schulmedizin und ermöglichen positive Effekte wie Entspannung, Wohlbefinden und die Verminderung von Nebenwirkungen konventioneller Behandlungen. Im dritten Studienjahr erhielten Studierende des Bachelor-Studiengangs Pflege im Rahmen eines einwöchigen Wahlmoduls Einblicke in diese und weitere komplementäre Behandlungsmethoden. Ziel Welche positiven Erfahrungen und persönlichen Bereicherungen haben die Studierenden durch die Teilnahme am Wahlmodul gemacht? Methode Im Wahlmodul erlernten die Studierenden theoretische und praktische Grundlagen verschiedener Heilmethoden wie Phytotherapie, Aromatherapie, Anthroposophische Medizin, Osteopathie, Hypnotische Kommunikation, Reiki und Märchen in der Pflege. Zudem wurden die traditionellen Methoden Gesundbeten und Schamanismus vorgestellt. Die Studierenden erlebten beispielswiese auch rhythmische Einreibungen, Wickel, Kompressen und Massagen am eigenen Körper. Zusätzlich besuchten sie das Zentrum für integrative Pädiatrie am Kantonsspital Freiburg. Resultate Die Evaluation zeigt, dass die Studierenden die vermittelten Inhalte als relevant und praxisnah bewerten. Die Qualität der Lehre wurde positiv eingeschätzt und die praktischen Anwendungen wurden sowohl für den beruflichen als auch privaten Alltag als wertvoll empfunden. Diese Rückmeldungen liefern wichtige Hinweise für die Weiterentwicklung des Moduls. Schlussfolgerung Das Wahlmodule «Integrative und komplementäre Behandlungsmethoden» macht in der konventionellen Ausbildung der Pflegefachpersonen den Unterschied. Es vermittelt den Studierenden fundierte Kenntnisse und praktische Fähigkeiten, die sie in ihrer beruflichen Praxis anwenden können. Mit den in diesem Wahlmodul erworbenen Kompetenzen sind die Studierenden in der Lage, Patientinnen und Patienten zu beraten und bestimmte komplementäre Behandlungsmethoden selbst anzuwenden. Besonders in der Palliative Care, wo das Ziel darin besteht, die Lebensqualität der Patientinnen und Patienten zu optimieren und ihnen umfassende Unterstützung zu bieten, sind diese zusätzlichen Fähigkeiten von grossem Wert. |
||
|
P42
Begleitung Kranker und Sterbender durch ein flächendeckendes Netzwerk von qualifizierten Freiwilligen
Martina Holder-Franz, Aarau CH
Abstract
Hintergrund
Im Kanton Aargau haben die drei Landeskirchen seit 2010 zahlreiche Freiwillige für die Begleitung von Kranken und Sterbenden ausgebildet. Entstanden ist ein unverzichtbarer tragender Dienst, in dem rund 170 Freiwillige im Kanton Aargau engagiert sind, organisiert in 13 Regionalgruppen. Die Einsatzzentrale, die 365 Tage im Jahr besetzt ist, wird professionell geleitet und vermittelt auf Wunsch schwer kranker Menschen und deren Angehörigen Begleitungen. Davon profitieren unentgeltlich alle Menschen, unabhängig von ihrer Religionszugehörigkeit. Ziel Ziel ist die kompetente Unterstützung und respektvolle Begleitung von schwerkranken Menschen und die Entlastung der pflegenden Angehörigen. Methode Definiertes Aus- und Weiterbildungsprogramm, definierte Bestimmungen zur Qualitätssicherung sowie dessen ständige Weiterentwicklung. Resultate Im Jahr 2024 wurden knapp 8500 Stunden Begleitdienst geleistet, das entspricht fast 24h pro Tag. In jeder Minute war demnach irgendwo im Kanton eine Person an einem Sterbebett und in der Begleitung einer chronisch kranken Person im Einsatz. 2022 hat die Fachhochschule Nordwestschweiz in einer Studie dieses Angebot wissenschaftlich untersucht und Ergebnisse veröffentlicht (Palliative Care und Begleitung: Ein Angebot der Aargauer Landeskirchen). Diskussion Mittlerweile werden Aus- und Weiterbildung, Fachtagungen und Veranstaltungen auch in Kooperation mit palliative aargau, SRK und Careum Weiterbildung angeboten, von denen auch die Freiwilligen profitieren. Schlussfolgerung Der Palliative Care Begleitdienst durch Freiwillige kann aufgrund der definierten Standards auf hohem Niveau angeboten werden. Er erfährt eine grosse Akzeptanz weit in die Gesellschaft hinein und wird von entsprechenden staatlichen Stellen wahrgenommen und zunehmend als tragend und wesentlich für die Versorgung beachtet. Im Sinne von "tue Gutes und rede darüber" möchten wir informieren und andere für die Freiwilligenarbeit motivieren. Daliah Koch, Einsatzleiterin Begleitdienst |
||
|
P43
Das Paediatric Palliative Care Network Schweiz (PPCN CH) – ein wirkungsstarker Zusammenschluss
Martin Höss, Horn CH
Abstract
Hintergrund
Das Schweizer Netzwerk von in der Pädiatrischen Palliative Care (PPC) tätigen Fachpersonen, setzt sich für Kinder mit lebensbedrohlichen und lebensverkürzenden Erkrankungen sowie deren Familien und anderen Nahestehenden ein. Es hat sich in den vergangenen 15 Jahren etabliert und ist zu einem festen Bestandteil bei PPC-tätigen Fachpersonen geworden, was die ungebrochen steigenden Mitgliederzahlen belegen (36 Einzel- und 75 Kollektivmitglieder aus 20 verschiedenen Organisationen (Stand 15.05.2025). Zu Beginn war das Netzwerk monoprofessionell aus Pflegefachpersonen mit unterschiedlichen Settings und ideellem ärztlichen Support organisiert. Von Anfang an war entscheidend, eine breite interprofessionelle Vertretung im Bereich der PPC zu gewährleisten insbesondere auch die Ärzteschaft. Ziel Ziel des Netzwerkes ist es, die gesamte Versorgungsstruktur abzubilden: der stationäre Bereich, ambulant Tätige in der Kinderspitex oder aus Organisationen, die sich mit Freiwilligen engagieren, Fachpersonen aus den Bereichen Psychologie, Körpertherapien, pädagogischen Institutionen, Hospiz-Initiativen, wie auch Seelsorgende, Sozialarbeitende, Fachpersonen in Bestattung, Trauerbegleitung und der Forschung. Methode Die Website des Netzwerkes ist in der Website von palliative.ch integriert und bildet so noch klarer die gemeinsamen Ziele sowie die nationale Vernetzung ab. Die Zusammenarbeit wird weiter ausgebaut, sei dies in Bezug auf den gemeinsamen Auftritt, das Einbringen von Schwerpunktthemen wie auch die Vertretung der pädiatrischen Anliegen und das Sichtbarmachen der PPC auf verschiedenen Kanälen. Den Mitgliedern steht auf der Website ein geschützter Bereich mit Zugang zu internen Dokumenten zur Verfügung. Resultate Die interprofessionelle Zusammenarbeit zeigt sich praktisch im Austausch der Fachpersonen, im Erarbeiten von gemeinsame Grundlagenpapieren, der Weiterbildung, optimiert durch ein eigenes Curriculum und Weiterentwicklung der Pädiatrischen Palliative Care in der Schweiz. Für die Öffentlichkeitssensibilisierung schliesst sich das Netzwerk zum vierten Mal der jährlichen internationalen Sensibilisierungskampagne «HatsOn4CPC-Day» für Pädiatrische Palliative Care an. Schlussfolgerung Die Qualität des Angebotes für und durch die Mitglieder hat sich seit der Gründung durch Strukturen, Angebote und Interprofessionalität verbessert. Als Orientierung für die Aktivitäten stehen die Bedürfnisse der Kinder im Fokus und die Bedürfnisse der Eltern werden einbezogen. Die Netzwerktreffen finden drei Mal pro Jahr statt. 
|
||
|
P44
Terminalphase: Empowerment der Familie
Shanaya Karpf, Winterthur CH
Abstract
Hintergrund
Familien sind für Menschen in der Terminalphase eine relevante Ressource und können den Sterbeprozess positiv beeinflussen. Der Einbezug von Familienmitglieder in die Pflege von sterbenden Personen kann die Selbstwirksamkeit der Familie positiv beeinflussen. Es können aber auch tiefe Trauer und Gefühle der Überforderung auftreten. Ziel Das Poster beschreibt, wie Pflegefachpersonen Familien in der Terminalphase im Akutspital unterstützen können. Methode Es wurde eine systematisierte Datenbankrecherche auf PubMed und CINAHL Complete durchgeführt. Resultate Studien weisen darauf hin, dass von Seiten der Pflegefachpersonen eine einfühlsame Herangehensweise vonnöten ist, insbesondere beim Ansprechen des bevorstehenden Sterbens. Die Familien können darin bekräftigt werden, Unterstützung und Tipps der Fachpersonen im Umgang mit der sterbenden Person (z.B. Berührung, Mundpflege) anzunehmen, aber auch, eigene Grenzen anzuerkennen bzw. Selbstpflege zu betreiben. Schlussfolgerung Das Empowerment von Familien in der Terminalphase durch Pflegefachpersonen bewegt sich zwischen den Polen der beratenden Unterstützung bei der Interaktion mit der sterbenden Person bzw. beim Anerkennen von Grenzen. |
||
|
P45
Benefit of a Modular Intervention to Promote Dignity, Meaningfulness and Mindfulnessin Acute Care
Katharina Klatte, Basel CH
Abstract
Hintergrund
Patients with life-limiting illnesses commonly experience substantial distress and loss of dignity. Relieving distress by fostering dignity and meaning have been identified as a core objective of palliative care. To address the individual needs of this heterogeneous patient group, we have developed a modular approach for the acute care setting consisting of Dignity Therapy, modified Managing Cancer and Living Meaningfully (CALM) Therapy, and a mindfulness-based intervention (MBI). Results of a previously performed feasibility study (n=10) showed high acceptance of the modular intervention and a strong benefit in the areas of dignity, meaning of life, and will to live. Ziel The aim of the present randomized controlled trial is to evaluate whether the modular intervention, in addition to standard specialized palliative care (SSPC), will promote dignity, meaningfulness, and mindfulness to a larger extent than SSPC alone. Methode 40 patients from the palliative care consulting service of the University Hospital Basel (life expectancy < 18 months) will be randomized to receive either the modular intervention and SSPC or SSPC alone. Patients in the intervention group can choose one of the offered modules. Each module consists of two sessions. Changes in mental well-being pre- versus post-intervention are measured by the PDI in both groups. Secondary outcomes include depressive symptom severity assessed with the Patient Health Questionnaire-9 (PHQ-9), the Integrated Palliative Care Outcome Scale (IPOS) and semi-structured interviews. Resultate Recruitment for RCT is ongoing. After study completion in October 2025 primary analysis will test the hypothesis by fitting a simple linear regression model, regressing the difference in scores on the treatment arm. Secondary outcomes as well as qualitative outcomes of the interview will be presented. Current qualitative outcomes of the feasibility study as well as the RCT intervention group show a high patient-perceived benefit of the modular intervention. Schlussfolgerung Results of this RCT will determine if the developed modular intervention constitutes a significant benefit for acute palliative care patients and merits implementation into routine practice. SAMW (PC28/17, PC 05/18) |
||
|
P46
Evaluation der evidenzbasierten Nachsorge für Angehörige in der spezialisierten Palliative Care
Myrta Kohler, Zürich CH
Abstract
Hintergrund
Die Betreuung einer nahestehenden Person mit terminaler Erkrankung und deren Tod stellen eine einschneidende und belastende Erfahrung dar, die sich erheblich auf die Gesundheit und das Wohlbefinden der Hinterbliebenen auswirkt. Klinische Leitlinien empfehlen ein dreistufiges Modell der „Bereavement Care“, um den unterschiedlichen Bedürfnissen der Angehörigen gerecht zu werden. Diese evidenzbasierten Empfehlungen wurden in der schweizerischen Palliativversorgung bislang nicht ausreichend berücksichtigt. Die BEST for Family-Studie stützt sich daher auf Methoden der Implementierungswissenschaft, um eine evidenzbasierte Nachsorge in zwei grösseren Schweizer Spitälern zu etablieren. Bestandteil sind unter anderem Telefonkontakte 3–6 Monate nach dem Verlust. Ziel Die Auswirkungen der Nachsorge auf die hinterbliebenen Angehörigen zu untersuchen. Methode Die Studie wird in einem konvergenten Mixed-Methods-Design durchgeführt. Untersucht werden die Angemessenheit, Kohärenz und Qualität des Programms sowie das Befinden der Angehörigen. Diese werden 3–6 Monate nach dem Verlust mittels Fragebogen befragt. Mit einem Teil der Teilnehmenden werden zusätzlich semistrukturierte Einzelinterviews geführt, um ein vertieftes Verständnis ihrer Erfahrungen und der Auswirkungen des Programms zu gewinnen. Die Datenanalyse erfolgt mittels deskriptiver und inferenzstatistischer Verfahren sowie einer induktiven Inhaltsanalyse. Resultate Bislang haben 17 Angehörige an der Datenerhebung teilgenommen, wovon mit 6 Personen vertiefende Interviews geführt wurden. Die Rekrutierung läuft bis Juli 2025 weiter; anschliessend werden die Daten vollständig analysiert. Erste Ergebnisse deuten darauf hin, dass die Interaktionen mit den Gesundheitsfachpersonen in der Sterbephase sowie das Nachsorgetelefonat mehrheitlich als hilfreich empfunden wurden, und sich die Angehörigen dabei verstanden fühlten. Schlussfolgerung Es sind empirische Erkenntnisse notwendig, die auf quantitativen und qualitativen Daten beruhen, um ein umfassendes Verständnis der Wirkung des neuen Nachsorgeprogramms zu gewinnen, um eine gezielte Weiterentwicklung zu ermöglichen, bevor es auf weitere Spitäler und Institutionen ausgeweitet wird. Dies gibt Hinweise auf zentrale Faktoren einer nachhaltigen Implementierung. Die Evaluation liefert somit wichtige Erkenntnisse zum Nutzen und zur Umsetzbarkeit im Schweizer Kontext aus Sicht der hinterbliebenen Angehörigen – ein bislang oft vernachlässigter Bereich. |
||
|
P47
Advance care plan: General Practitioner's advocacy as a must for patients in geriatric nursing homes
Jean-Claude Leners, Ettelbruck LU
Abstract
Hintergrund
Since the mid 80s, advance care plans (ACP) have been established as a tool to communicate formally patient's personal wishes in case of a chronic or acute medical disease, an accident or regarding end-of-life care. Some countries have started legalizations for 15 years. Our national plan on end-of-life stated to establish a medico-ethical consultation prior to fill in an ACP. Ziel This consultation must be well chosen : after a recent medical diagnosis (which might be acute, chronic or even life-threatening), after the loss of a family member and of course in a palliative care approach (oncological or not). A specific pricing has been elaborated and our GPs are encouraged to advocate for their patients in order to discuss firmly with them on a written form of ACP in nursing homes. (or even prior to admission) Methode In a recent study in Europe on ACP and treatment limitation, on admission, even in acute geriatric wards, only 5% respectively 14% had these documents in Western Europe. Our GP's advocacy for this written document should be one or several medico-ethical consultation(s) including: the patient, GPs and maybe other medical specialists, nurses and family members, but always centred on the patient's wishes. Resultate To give the patient the broadest possible neutral information on pros and cons, we have summarized this in a "SWOT analyses for ACP" in form of a flyer for patients preparing to the medico-ethical consultation 1) Strength = self-determination or autonomy and decision-making competence ( as golden standard for personal decisions); 2) Weakness = the best moment to discuss and write an ACP can be missed or maybe no surrogate has been designated at time ; 3) Opportunity = organizing one own's future in discussions with the doctors and family and not shifting the responsibility on others: 4) Threat = pressure from outside can result in inner conflicts of emotions and patients may renounce to fill-in an ACP or they are no longer able to express their own wills, when the oncological or neurological disease was too fast progressing. Schlussfolgerung For the GPs it is a unique chance to initiate this process and so patients in nursing homes can express their decisions on ACP. Nonetheless in homes , the major diagnosis of dementia will always be a challenge, because this disease can impair patient's mental capacity to decide on their own's future. |
||
|
P48
Bildungsangebot Lehrgang A2 Palliative Care für Menschen mit Beeinträchtigung
Katharina Linsi, Weinfelden CH
Abstract
Hintergrund
Im Rahmen der UNO-Behindertenrechtskonvention haben Menschen mit Beeinträchtigung verbindliche Rechte bekommen, insbesondere auch das Recht auf Selbstbestimmung am Lebensende.
Ziel Mit dem Start des A2 Kurses in Anlehnung an die Bildungsstruktur von palliative ch, sollen Institutionen für Menschen mit Beeinträchtigung für das Thema Palliative Care sensibilisiert werden. Der Bildungsbedarf soll erkannt und in der Folge entsprechende Weiterbildungsangebote entwickelt und etabliert werden.
Methode
Resultate Der erste 5 - tägige Lehrgang fand vom 17. März bis am 13. Mai 2025 in Weinfelden statt. Die Rückmeldungen der Teilnehmenden waren durchwegs positiv und bestätigten den Bedarf. Diskussion Wie können Institutionen auf Palliative Care sensibilisiert werden? Welche Strukturen braucht es, um den Bildungsbedarf systematisch zu erfassen und Angebote gezielt zu entwickeln? Schlussfolgerung Bildungsangebote im Bereich Palliative Care müssen auf die spezifischen Bedürfnisse von Institutionen für Menschen mit Beeinträchtigung zugeschnitten sein. Eine koordinierte Angebotsgestaltung unter Vermeidung von Doppelspurigkeiten ist zentral. Das entwickelte Schulungskonzept eignet sich zur Anwendung in weiteren Regionen der Deutschschweiz. 

|
||
|
P49
Palliative care integration for patients with end-stage renal disease: still work in progress?
Monika Lopez - Grossenbacher, Bellinzona CH
Abstract
Hintergrund
Patients with end-stage renal disease may have a significant symptom burden and complex co-morbidities. Palliative care (PC) can provide support to patients, their families and nephrology teams, but is rarely integrated within standard renal care. This is especially important for patients on a conservative kidney management (CKM) plan not undergoing dialysis Ziel The aim of this work is to integrate PC within standard renal care for patients undergoing CKM through a collaborative approach between nephrology and PC services.
Methode The starting point for shared discussions was a clinical case of a 58-year-old patient who chose not to be dialysed. This experience of the nephrology team led to reflections on the role PC could play throughout the disease trajectory of these patients. Guided by the EPIS (Exploration, Preparation, Implementation and Sustainment) framework, the develop-ment of a collaboration between the nephrology and the PC team was started. The key element of this ongoing process was a joint workshop on CKM and PC, organised by the nephrology team.
Resultate A total of 27 participants (3 from the PC and 24 from the nephrology team) joined the interprofessional workshop. Nurses and physicians benefitted from theoretical inputs about PC in CKM and from the lived experience of the aforementioned patient and his wife, who participated in the discussions. Furthermore, the PC team explained how to identify patients with PC needs through a structured identification tool. Emerging themes highlighted as priority for PC integration were the need for training in communication techniques, improved symptom management and better advance care planning.
Diskussion
Schlussfolgerung PC integration within CKM needs to address the key issues identified in the workshop, while fostering a holistic approach within the nephrology team that focuses on needs, symptoms and early planning to guarantee an appropriate quality of life of patients and their families. |
||
|
P50
Coordination of patients suffering from ALS followed by the multidisciplnary consultation
Floriana Lurati, Lausanne CH
Abstract
Contexte
In the context of amyotrophic lateral sclerosis (ALS), coordinated multidisciplinary care has been shown to improve quality of life and survival of patients. In the context of an ambulatory multidisciplinary consultation in a Swiss University Hospital, two major problems have been identified: (i) a too long delay between diagnosis and the start of treatment, and (ii) the presence of many healthcare providers in the community, making coordination difficult. Objectiv A survey has been launched by this consultation to take stock of the difficulties and needs of patients, family caregivers, and healthcare providers within and outside the hospital. Méthode The project was carried out in two phases: (i) creation of a database of patients, family caregivers and healthcare providers, and (ii) distribution of a questionnaire for these target populations. Résultats In total, 14 ALS patients, 12 family caregivers and 102 professionals completed the survey. Results underlined the importance of a better coordination for improving care. The survey particularly revealed gaps in professionals' specific knowledge and caregiver burnout. From that point, the priorities identified to improve the system were (i) identifying a pivotal person to centralize the patient's clinical follow-up, (ii) creating a shared care plan, and (iii) updating an anonymized database of patients and healthcare providers. Conclusion To ensure that these priority objectives are met, a position of clinical coordinator has been created to shorten the time between diagnosis and multidisciplinary follow-up and ensure smooth transitions. ALS training has also been set up for healthcare providers by this coordinator. In addition, initiatives are underway to create a steering committee to support the project at a regional level and to obtain the recognition of the ambulatory multidisciplinary consultation as a reference ALS center. Over time, this should enable us to strengthen cooperation between the healthcare providers of the community and the ambulatory multidisciplinary consultation. |
||
|
P51
iDecide: The Advance Directive App - Advance Care Planning in Pocket Format.
Maud Maessen, Bern CH
Abstract
Hintergrund
Advance Directives (AD) are central to Advance Care Planning (ACP). Despite broad public awareness and support, only one-fifth of the Swiss population has completed an AD. The roadmap for ACP implementation by the Swiss National Task Force ACP calls for the development of digital applications to promote ACP in Switzerland. While various online forms for AD creation exist, no mobile app has previously enabled the public to complete an AD. This study details the development process of the mobile application ‘iDecide’ (www.iDecide.ch) for AD creation, based on the Swiss Medical Association (FMH) AD template (short version). Ziel IDecide development followed a participatory action research (PAR) approach. The primary aim was to ensure optimal usability and user satisfaction with the iDecide app. Methode Following PAR, four iterative development cycles were conducted to create an evidence-based AD creation tool. The iDecide app, published in October 2024, was then critically reviewed by users through an online survey as part of the app. In this phase, the tool is limited to the German language. The survey evaluated the app’s user-friendliness, educational information quality, and concordance with ACP goals, measuring 14 items on a 5-point Likert scale. Resultate iDecide combines multimedia patient information on the content and value of AD, encourages reflection on personal preferences (spiderweb-diagram), and promotes communication with surrogate decision-makers and healthcare professionals (Figure 1). The final document is available in print and digital formats via an offline QR code. This QR code allows AD information to be stored on a personal device, shared, and accessed when needed. Data safety was positively evaluated by legal testing. Survey responses from 94 app users indicated high usability, information quality, and user satisfaction. On a five-star rating system, the mean overall rating was 4.69 (SD = 0.57, 95% CI: 4.56–4.81), consistent across age groups. Users rated the app as easy to use and making AD creation more attractive. Schlussfolgerung iDecide is a ready-to-use AD application, freely available to the public. The tool aligns with the national roadmap for ACP implementation and effectively tackles barriers to widespread AD implementation in Switzerland, addressing engagement and accessibility issues. As such, IDecide has the potential to empower individuals to actively engage in ACP. 
|
||
|
P52
Palliative Care@home: providing a sense of security through video consultations?
Maud Maessen, Bern CH
Abstract
Hintergrund
The ability of patients in palliative care to remain at home as long as possible is heavily dependent on the available ambulant care providers and the support provided by family caregivers. Acute medical deteriorations frequently result in uncertainty among family caregivers, which can lead to hospitalisation that might otherwise be avoidable through timely access to specialist palliative care (SPC) and proactive emergency planning. A sustained sense of security at home is essential for the successful implementation of Palliative Care at Home (PC@home). Despite its potential advantages, telemedicine remains underutilized in SPC within Switzerland. This is particularly noteworthy given its potential to reduce travel time and enhance access to SPC for family caregivers and patients with limited mobility, too sick to travel or those residing in remote areas. Ziel This project aims to instruct patients and their family caregivers in the use of a digital communication tool during hospitalization, helping them become better prepared to use it after discharge for prompt SPC consultations. It seeks to evaluate the implementation of this approach and assess its impact on caregivers’ perceived sense of security. Methode The study is structured as follows: Baseline Assessment: Questionnaires, including the “Sense of Security in Care” instrument for family caregivers. Face-to-Face Training: Support in the use of the video communication tool for both patients and caregivers by nurses. Video Consultation: Conducted 14 days post-discharge or as clinically indicated by SPC team. Follow-Up Assessment: Conducted 14 days after the video consultation, involving questionnaires and qualitative interviews with family caregivers. Focus Group: Collection of experiential data from participating physicians. Resultate As this is an ongoing study, preliminary findings will be presented at the conference. Schlussfolgerung This project holds significant potential to benefit patients, family caregivers, and healthcare professionals by: Enhancing equitable access to SPC for individuals with limited mobility, those living in rural areas, and caregivers who are geographically distant. Providing SPC team members with feedback on their video consultations, thereby supporting the delivery of high-quality PC@home. |
||
|
P53
Who Cares? Characteristics of Neighbours willing to provide Informal End-of-Life Support.
Maud Maessen, Bern CH
Abstract
Hintergrund
Switzerland is experiencing a demographic shift, with a rapidly aging population and increasing demand for end-of-life care at home. Formal care systems alone are insufficient to meet this need, making informal caregivers—family, friends, and neighbours—essential. The Compassionate Communities movement promotes community-based support for people facing serious illness, dying, and loss. Ziel This study aimed to identify the characteristics of individuals who are not only willing but also have demonstrated behavioural engagement to provide informal, voluntary support to neighbours at the end of life. Methode A cross-sectional survey was conducted during two public events in Bern: a football match and the city festival endlich.menschlich.. Participants completed a 29-question survey assessing demographics, prior caregiving experience, and willingness to support neighbours in hypothetical end-of-life scenarios and signing up for a database of volunteers who want to support their neighbours. Resultate Of 828 completed questionnaires, 134 respondents signed up for volunteering and were included in the analysis. Among the 134 respondents, 72% were female, 48% were aged 40–64, and 65% had tertiary education. Most were employed (62%) and married or in a domestic partnership (48%). A significant proportion had prior experience in voluntary work (83%) and/or the healthcare sector (59%). Schlussfolgerung The study highlights a core demographic of the primary group not only willing to engage in informal end-of-life care in their neighbourhood, but also showing active behaviour. These insights provide a valuable baseline for future research and program development as Bern continues to evolve as a Compassionate City. The results also support the Bern Declaration’s call to recognize and empower informal caregivers (www.phpci.org/berndeclaration). Targeted outreach, education, and support are essential to sustain and expand these community-based networks. |
||
|
P54
Les soins palliatifs précoces en EMS : une nouvelle dimension des soins de base?
Vener Marco, Russo CH
Abstract
Hintergrund
Au Tessin les Soins Palliatifs Gériatriques (SPG) sont considérés des soins spécialisés et la réponse au besoin issue de ces soins confie à une quarantaine de lits répartis sur cinq EMS. Mais les données que nous avons récoltées au cours nos pratiques nous montrent une tout autre réalité. En 2023 nous avons présenté au congrès national de Bienne une analyse de la prévalence du besoin en soins palliatifs dans la population de patients gériatriques qui vivent dans les deux EMS qui nous gérons. En 2025 nous avons déterminé avec ID-Pall la Prévalence du besoin en soins palliatif des patients nouveaux l’arrivée dans nos institutions. En 2022 nous avons obtenu la certification fédérale en qualité pour les soins palliatif. Ziel Déterminer la Prévalence du Besoin en soins palliatifs des patients nouveaux admis dans un EMS et évaluer si considérer les SPG précoces comme de soins de base. Methode Dans le but de définir un échantillon de patients non exposé aux pratiques de notre l'institution, nous avons décidé d'administrer l'ID-PALL après un minimum de 7 jours et un maximum de 14 jours à tout nouveau patient admis dans nos services entre le 1.1.25 et le 31.3.25 (N = 14). Parmi ceux-ci, les facteurs de complexité spécialisée sont identifiés par ID-PALL. Resultate 100% des patients nouveau admis ont besoin de SP dont 71% ont besoin de SP spécialisé. Les caractéristiques des besoins spécialisés sont: 30% du total présentent au moins un symptôme grave et persistant qui ne répond pas dans les 48; 60% du total présentent une souffrance psycho sociale du résident; 30% du total présentent une souffrance psycho sociale de la famille; 30% du total nécessitent d'une sédation palliative; 60% du total ont des difficultés à planifier soins et/ou directives. Dans 40% du total des cas, le soutien de la deuxième ligne a été mis en œuvre immédiatement. Schlussfolgerung La prévalence du Besoin en soins palliatif chez le patient gériatrique nouveau admis en EMS est très élevée. Les résultats de 2025 confirment les résultats de Prévalence présentés en 2023. Ainsi nous considérons que les SPG précoces sont des soins de base que nos EMS doivent garantir à tous les patients. Nous devons donc nous assurer que la réponse à ce Besoin soit la plus efficace possible. Un design de recherche pour la mesure des effets de notre réponse est ainsi en préparation. |
||
|
P55
Nichtmedikamentöses Management von Dyspnoe bei palliativen Krebspatient:innen mit dem Handventilator
Luca Märki, Winterthur CH
AbstractHintergrund Dyspnoe ist eines der häufigsten Symptome bei Patient:innen mit fortgeschrittenen Tumorerkrankungen. Die Prävalenz liegt zwischen 10-70%. Eine Reduktion der Dyspnoe führt zu verbesserten Atemfunktionen, erhöhter physischer Leistungsfähigkeit und gesteigerter Lebensqualität. Daher ist eine suffiziente Symptombehandlung – u.a. durch nichtmedikamentöse Interventionen - essenziell. Ziel Das Poster beschreibt, wie die nichtmedikamentöse Intervention des Handventilators das Management von Dyspnoe bei Krebspatient:innen im palliativen Setting unterstützen kann. Methode Es wurde eine systematisierte Datenbankrecherche auf PubMed und CINAHL Ultimate durchgeführt. Resultate Die Intervention Handventilator weist verglichen mit anderen nichtmedikamentösen Interventionen zum Management von Dyspnoe bei palliativen Krebspatient:innen die beste Evidenz auf. Entsprechend wird diese Intervention (Anwendung, Vor-/Nachteile) vorgestellt und diskutiert. Schlussfolgerung Dyspnoe kann ein häufiges und belastendes Symptom bei Krebspatient:innen sein, dessen Management einen multimodalen Ansatz erfordert. Nichtmedikamentöse Interventionen wie die Anwendung eines Handventilators stellen dabei eine wichtigen Pfeiler des Symptommanagements dar. |
||
|
P56
Equipes mobiles de soins palliatifs : Développer la valorisation des compétences des accompagnants spirituels
Anne-Sylvie Martin, Rennaz CH
Abstract
Contexte
Pour la prise en charge palliative, le canton de Vaud est partagé en 4 régions de santé et une équipe mobile de soins palliatifs pédiatriques ; depuis 2023, les Eglises catholique et protestante ont mis un accompagnant spirituel (AS) à disposition de chaque équipe mobile de soins palliatifs. Objectiv Nous souhaitons vous détailler la méthodologie d’intervention (sous la forme d’un vademecum) de ces accompagnants spirituels d’un nouveau style et la posture métier qu’ils sont en train de co-construire avec les soignants. Méthode
1.Début de la prise en soins spirituels
2.Prise en soins spirituels
3.Fin de la prise en soins spirituels
4.Collaborations en équipe interprofessionnelle
Résultats
Conclusion L’objectif de rendre compte de la pratique actuelle des AS EMSP sous forme écrite a permis :
|
||
|
P57
Interprofessionelles Team - auch in der ambulanten spezialisierten Palliative Care
Marlene Matzinger, St.Gallen CH
Abstract
Hintergrund
Der Palliative Brückendienst (PBD) der Krebsliga Ostschweiz ist ein mobiler, spezialisierter Palliative Care-Dienst, der überregional schwerkranke, sterbende Menschen, deren Angehörige sowie Fachpersonen in palliativen Situationen in Zusammenarbeit mit der Grundversorgung betreut und zu physischen, psychologischen, sozialen und spirituellen Problemen berät. Der PBD arbeitet basierend auf einem nurse-led Konzept, bei dem Pflegefachpersonen Besuche vor Ort leisten, für medizinische Fragen stehen Palliativärztinnen/-ärzte telefonisch zur Verfügung. Bislang fehlte in der spitalexternen Grundversorgung ein Vorgehen, um komplexen palliativen Situationen sowie spirituellen Bedürfnissen vor Ort interprofessionell zu begegnen. Im neuen Angebot "PalliativMobil" führen eine PBD-Pflegefachperson und eine Palliativärztin interprofessionell Besuche vor Ort durch. Im Projekt "Ambulante Spiritual Care" wird ein Team bestehend aus Pflegefachpersonen und spezialisierten Seelsorgenden vom PBD für die spirituellen Bedürfnisse von Menschen in palliativen Situationen und deren Angehörigen beigezogen. Ziel Ziel des Projekts ist, die Einsätze von "PalliativMobil" und "Ambulante Spiritual Care" wissenschaftlich zu begleiten. Methode Die wissenschaftliche Begleitung von "PalliativMobil" (2024-2026) basiert auf einem qualitativen, multiperspektivischen Ansatz, der das Ausfüllen von Tätigkeitsprotokollen, die Durchführung von Einzel- und Fokusgruppeninterviews und die Erstellung "finanzieller Cases" beinhaltet. Die Einsätze von "Ambulante Spiritual Care" werden mittels Tätigkeitsprotokollen evaluiert. In beiden Projekten werden die synthetisierten Erkenntnisse in einem mehrstufigen Prozess diskutiert und Empfehlungen zur Fortführung formuliert. Resultate 184 ausgefüllte Tätigkeitsprotokolle zu "PalliativMobil" bzw. 20 zu "Ambulante Spiritual Care" sowie vier Workshops zeigen bislang auf, dass interprofessionelle Zusammenarbeit den fachlichen Austausch sowie die ganzheitliche Betreuung in komplexen palliativen Situationen im ambulanten Setting fördert. Schlussfolgerung Erste Erkenntnisse unterstreichen, dass eine koordinierte und vernetzte interprofessionelle Zusammenarbeit in der ambulanten spezialisierten Palliative Care zu einer qualitativ hochstehenden Betreuung und Begleitung von Betroffenen, Angehörigen und Fachpersonen beiträgt, den Edukationseffekt in der Grundversorgung stärkt und das gesundheitspolitische Konzept "Ambulant vor Stationär" unterstützt, indem Krankenhausaufenthalte verkürzt oder vermieden werden. |
||
|
P58
Craniosacral Therapie in einem palliativen Setting – Erfahrungen, Potenziale, Herausforderungen
Stefanie Mey, Winterthur CH
Abstract
Hintergrund
Die Craniosacral Therapie (CST) ist eine anerkannte Methode der Komplementärtherapie, die das autonome Nervensystem reguliert, Schmerzen lindert, emotionale Stabilität fördert und das Körperbewusstsein stärkt. Im Rahmen einer Diplomarbeit wurde CST auf der Palliativstation eines Akutspitals eingesetzt. Ziel Ziel war es, Nutzen, Akzeptanz und mögliche Wege einer nachhaltigen Integration zu evaluieren. Methode Während zwei Monaten nahmen insgesamt 15 Patient:innen an 16 Sitzungen teil. Die Rekrutierung der Patient:innen erfolgte über das interprofessionelle Team anhand festgelegter Kriterien, mit anschließender mündlicher und schriftlicher Einwilligung. Die Dokumentation umfasste medizinische und personenbezogene Daten, Behandlungsziele sowie Patienten rapportierte Outcomes (PROMs). Resultate Die Rückmeldungen von Patient:innen sowie dem interprofessionellen Team waren positiv. Besonders geschätzt wurden der ganzheitliche Ansatz und die Dauer von 60 Minuten pro Sitzung, welche Raum für individuelle Bedürfnisse und tiefergehende therapeutische Prozesse bot. CST wurde als wirksam in der Symptomlinderung, Förderung von Wohlbefinden und Unterstützung psychosozialer Themen erlebt. Auf der Visuellen Analogskala bewerteten alle Patient:innen ihre Leitsymptome um durchschnittlich drei Punkte geringer. Die CST scheint insbesondere auf Schmerzen, Angst und Atemnot einen positiven Einfluss zu haben, welches auch bessere funktionale und partizipative Fähigkeiten zur Folge hat. Die Wirksamkeit der um CST ergänzten interprofessionellen Behandlung kann durch die PROMs-Messung mit der integrierten Palliative Care Outcome Scale (IPOS) erwiesen werden. Trotz positiver Erfahrungen stellen sich wesentliche Herausforderungen bei der Implementierung: CST ist derzeit an die ausgebildete Einzelperson gebunden, nicht regulär abrechenbar und nicht im Leistungskatalog des Spitals verankert. Die Weiterentwicklung umfasst die Bekanntmachung der Resultate, interne und externe Netzwerkbildung, sowie Öffentlichkeitsarbeit. Perspektivisch zeigt sich CST als bereichernde Ergänzung in der palliativen Versorgung. Schlussfolgerung Diese Arbeit zeigt, dass CST unter professionellen Bedingungen einen messbaren Mehrwert für Patienten bietet und zur Ergänzung der medizinischen Versorgung beiträgt. Eine interprofessionell abgestimmte Implementierung – gestützt durch klinische Erfahrung, evidenzorientierte Evaluation und strukturelle Verankerung – ist der Schlüssel für eine Integration komplementärtherapeutischer Angebote im Spital. |
||
|
P59
Mitgefühl in Palliative Care Pflegeteams fördern – Möglichkeiten und Grenzen
Julia Müller, Zürich CH
Abstract
Hintergrund
Mitgefühl ist die Fähigkeit, einem Menschen in belastenden Situationen hilfreich zur Seite zu stehen. Es gilt als zentrales Prinzip der Palliative Care, das nicht nur eine wesentliche Rolle für die interprofessionelle Versorgungsqualität, sondern auch für die Gesundheit der Health Professionals spielt. Trotzdem wird Mitgefühl in der Gesundheitsversorgung oft durch ökonomische und bio-medizinische Faktoren in den Hintergrund gedrängt und dadurch seine Integration in die Praxis erschwert.
Ziel Ziel der Arbeit war Faktoren zu identifizieren, die Mitgefühl in Palliative Care Pflegeteams im klinischen Kontext stärken.
Methode Die Fragestellung wurde anhand des aktuellen Forschungsstandes bearbeitet. Die Ergebnisse wurden im Sinne einer kommentierten Validierung in leitfadengestützten Gesprächen mit drei Fachexpert:innen der Praxis vertieft und diskutiert. Resultate Mitgefühl darf nicht lediglich als persönliche Fähigkeit verstanden werden. Es stellt eine professionelle Kompetenz dar, die unter bestimmten Bedingungen entwickelt werden kann. Voraussetzung dafür sind ein gemeinsames Begriffsverständnis, begünstigende Einflussfaktoren und die Planung von Mitgefühl fördernden Interventionen. Als Einflussfaktoren wurden persönliche, teambezogene und strukturelle Aspekte identifiziert. Diskussion Die Palliative Care wird wesentlich durch das Mitgefühl der Pflegefachpersonen getragen. Auch wenn Mitgefühl teils mit traditionellen Rollenbildern assoziiert und daher mit Vorbehalt betrachtet wird, zeigt sich sein emanzipatorisches Potenzial: Es betont die eigenständige Kultur, Ethik und Kompetenz der Pflege. Mitgefühl ist eine inhärente Qualität, die durch Selbstfürsorge und gezielte Impulse gestärkt werden kann. Da es stets in Beziehung entsteht, braucht es Räume zur gemeinsamen Reflexion und eine mitfühlende Teamkultur. Solange entsprechende Bemühungen nur auf Teamebene erfolgen, bleiben sie begrenzt wirksam. Nachhaltige Förderung braucht auch strukturelle Lernangebote und geeignete Rahmenbedingungen. Schlussfolgerung Auch unter begrenzten strukturellen Voraussetzungen können Pflegeteams Mitgefühl gemeinsam stärken. Ansatzpunkte finden sich in der Gestaltung eines unterstützenden Teamklimas sowie in gemeinsamen Reflexions- und Lernprozessen im Pflegealltag. Die Arbeit leistet einen Beitrag zur Verankerung von Mitgefühl als kollektive, reflektierte Haltung in Palliative Care Pflegeteams und bietet Impulse für praxisnahe Entwicklungsmassnahmen. |
||
|
P60
Einsatz der Serial Trial Intervention (STI) bei herausfordernden Verhaltensweisen in der palliativen Geriatrie.
Veronika Müller, Mauren FL LI
Abstract
Hintergrund
Herausfordernde Verhaltensweisen von Menschen mit Demenz (MmD) in Langzeiteinrichtungen belasten Pflegepersonal und Bewohnende erheblich. In den Pflegeheimen der LAK wurde die Serial Trial Intervention (STI) eingeführt, ein strukturiertes Instrument zur Identifikation zugrunde liegender Bedürfnisse und Reduktion herausfordernder Verhaltensweisen. Im Kontext der Palliativen Geriatrie hat die Anwendung der STI nicht nur Einfluss auf die Pflegequalität, sondern auch auf die Lebensqualität der Bewohnenden. Ziel Ziel war es, die Implementierung und Wirksamkeit der STI zu evaluieren und zu untersuchen, wie Pflegefachpersonen diese zur Reduktion herausfordernder Verhaltensweisen einsetzen. Besonders im palliativgeriatrischen Kontext wurde die Relevanz der STI für die Lebensqualität der MmD untersucht. Methode Zur Untersuchung der STI-Nutzung wurde eine Online-Befragung unter Pflegefachpersonen der Spezialstationen für Demenz durchgeführt. Es wurden Fragen zur Anwendung der STI, zu Schrittabfolgen und unterstützenden Hilfsmitteln gestellt. Die gewonnenen Daten wurden qualitativ und quantitativ ausgewertet, um die Wirksamkeit und Optimierungspotenziale der STI zu identifizieren. Resultate Die Ergebnisse zeigten eine hohe Akzeptanz und Wirksamkeit der STI bei der Reduktion herausfordernder Verhaltensweisen, besonders bei der frühzeitigen Identifikation von Schmerzen, was im palliativgeriatrischen Kontext besonders wichtig ist. Weitere Potenziale wurden in der verstärkten Anwendung bei weniger auffälligen Verhaltensweisen wie Apathie und Depression sowie der stärkeren Einbindung von Angehörigen und Hausärzten identifiziert. Schlussfolgerung Die STI ist ein effektives Instrument zur Verbesserung der Lebensqualität von MmD im palliativgeriatrischen Kontext. Zukünftige Anwendungen sollten zusätzlich auf weniger auffällige Verhaltensweisen und eine intensivere Zusammenarbeit mit Angehörigen und Fachpersonen fokussieren. 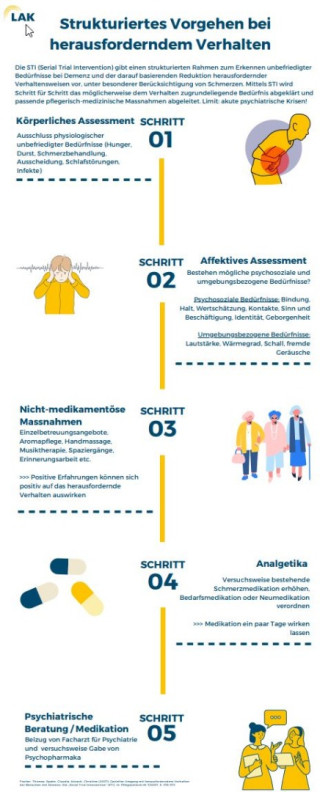
|
||
|
P61
Brücken bauen für sichere Übergänge: integrierte Palliative Care als regionales Versorgungsmodell
Birgit Nägeli, Hasle-Rüegsau CH
Abstract
Hintergrund
Menschen, welche sich in palliativen Krankheitssituationen befinden, erleben oft wiederholte Wechsel zwischen Spital und zu Hause. Diese Spitaleinweisungen treten dann auf, wenn daheim die Symptome nicht ausreichend kontrolliert werden können oder das Netzwerk die belastende häusliche Betreuung nicht mehr gewährleisten kann. Wenn Patient*innen in instabilen und komplexen Krankheitssituationen nach Hause austreten wollen, braucht es ein interprofessionelles Team, die Befähigung der Angehörigen sowie Fachexpertise, um diese Übergänge sicher zu gestalten, die Symptome gut zu kontrollieren und das Netzwerk zu stärken. Projekt: Der Kanton Bern hat in seiner Gesundheitsstrategie Teilstrategien erarbeitet, darunter die «Integrierte Versorgung» und «Palliative Care». Die seit 2021 bestehende Kooperation zwischen dem Spital Emmental und dem mobilen Palliativdienst Emmental/Oberaargau (mpdEO) verbindet diese beiden Teilstrategien. Die leitende Palliativmedizinerin der spezialisierten Palliative Care (SPC) im Spital ist zusätzlich die ärztliche Leitung des mpdEO. Zudem arbeitet eine Advanced Practice Nurse (APN) neben ihrer Anstellung in der SPC in einer Brückenfunktion im mpdEO. Ziel Ziele dieser integrierten Versorgung und interprofessionellen Zusammenarbeit sind (a) die Verbesserung der Patienten- und Angehörigenbetreuung in komplexen, palliativen Krankheitssituationen (b) die Verbesserung des Austrittsmanagements der Patient*innen dank dem Angebot einer Brückenfunktion zwischen Spital und mpdEO (c) die Stärkung des Netzwerkes von Betroffenen und ihren Angehörigen Methode Qualitätssicherungsprojekt zur integrierten Versorgung mittels Durchführung von: (a) gemeinsamen Rundtischgesprächen im Spital mit Patient*in, Angehörigen, Team der SPC und mpdEO vor einem Austritt nach Hause (b) gemeinsamen interprofessionellen und -disziplinären Patientenbesuche zu Hause oder in der palliativmedizinischen Sprechstunde im Spital. Resultate Erste informelle Rückmeldungen von Patient*innen und Angehörigen zeigen, dass sie sich beim Austritt nach Hause sicher betreut fühlen. Die Zusammenarbeit ermöglicht eine frühzeitige Symptomkontrolle und Netzwerkstabilisierung. Folgende Herausforderungen des Projekts können bisher identifiziert werden:
Schlussfolgerung Nächste Schritte bestehen in der systematischen Erfassung der Rückmeldungen von Patient*innen und Angehörigen. |
||
|
P62
An outpatient neuropalliative care clinic for patients with amyotrophic lateral sclerosis
Letizia Panicari, Bellinzona CH
Abstract
Contexte
Background: Neuropalliative care (NPC) is an emerging field of medicine focused on improving quality of life for patients and their caregivers living with serious neurodegenerative diseases. Evidence-based practices on how to best integrate palliative care (PC) into neurology is limited. Objectiv Aim: We here describe the model of our outpatient NPC clinic for patients with amyotrophic lateral sclerosis (ALS). Méthode Methods: Guided by the Exploration and Preparation phases of the Exploration, Preparation, Implementation, and Sustainment (EPIS) framework, we developed a detailed implementation plan. We analyzed the clinical peculiarities of the outer context (patients with ALS and their caregivers), the inner context variables within our institution, the innovation factors (the neurologic setting with unique PC needs) and the bridging factors (the holistic approach to care focusing on a person's emotional, spiritual, as well as physical and psychosocial needs). Résultats Results: We implemented an integrated model of PC where we share the same space: the average patient comes to clinic once every 3 months. During a joint visit, patients meet as a standard of care an NPC physician together with a neurologist and a nurse specialized in neuromuscular diseases. The same day, selected patients meet a pulmonologist specialized in mechanical ventilation. Every 3 months we have multidisciplinary meetings with nutritionists, social workers, physiotherapists (for respiratory and physical therapy), occupational therapists, home-based PC team, and representatives of the local ALS Association. Patients can also be referred to see a geneticist, a speech therapist, a spiritual care provider and a psychologist. Patients requiring inpatient care can be directly admitted in our acute specialist PC unit.
Conclusion Conclusion: With the implementation of our outpatient NPC clinic, we aim to address the clinical and public health needs of patients with ALS and their caregivers through the incorporation of advanced care planning into neurological patients’ routine care. |
||
|
P63
Wir machen einen Unterschied: Soziale Arbeit in der ambulanten Palliative Care
Susanne Pauli, Zürich CH
Abstract
Hintergrund
Menschen mit lebenslimitierenden Erkrankungen sind sehr herausgefordert. Betroffene, die nur begrenzte finanzielle Mittel zur Verfügung haben oder aus anderen Gründen sozial benachteiligt sind, erleben eine Mehrfachbelastung, die ihr Leiden und das ihrer Angehörigen massiv verstärken können. In der pädiatrischen Palliative Care (PC) zeigt sich, dass Sozialarbeitende durch die Erschliessung von finanziellen Mitteln und weiteren Ressourcen, die Beratung in sozialrechtlichen Fragen und durch die psychosoziale Begleitung im Umgang mit dem Sterben zur Lebensqualität und zur Wahrung der Autonomie beitragen. Sie sind daher fester Bestandteil der pädiatrischen palliativen Betreuung - auch im ambulanten Setting. Bei den Erwachsenen sind Sozialarbeitende zwar in Spitälern weitgehend gut etabliert, in der ambulanten PC aber kaum vertreten trotz dem Ausbau ambulanter Betreuungsstrukturen. Ziel Mit dem Qualitätsprojekt werden Chancen und Herausforderungen aufgezeigt, die sich für eine umfassende Betreuung und Begleitung von schwerkranken Menschen ergeben, wenn spezialisierte Sozialarbeitende in die ambulante Palliativversorgung eingebunden sind. Ziel ist es, erste Erfahrungen mit alternativen Versorgungsansätzen zu vermitteln, um den Weg für eine dauerhafte Etablierung von Sozialarbeitenden in der ambulanten Palliativversorgung zu bereiten. Methode Vorstellung der aktuellen Versorgungsstrukturen ambulanter Sozialarbeit im Kanton ZH, beispielhafte Darstellung und Kommentierung erfolgter ambulanter Begleitungen durch die Soziale Arbeit in Zusammenarbeit mit den spezialisierten Palliativspitexorganisationen und der Palliativseelsorge. Aufzeigen von typischen Themen der sozialarbeiterischen Bearbeitung sowie Herausforderungen, die sich durch die spezifische Versorgungsstruktur ergeben. Resultate Betroffene bringen zwar ihre Erleichterung zum Ausdruck, Unterstützung in sozialarbeiterischen Belangen zu erhalten. Die sehr begrenzte Verfügbarkeit der Sozialen Arbeit im ambulanten Setting im Kanton ZH wirft aber Fragen auf betreffend die Ressourcengerechtigkeit gegenüber Sterbenden, die keinen Zugang zu dieser Dienstleistung haben. Andererseits lässt sich die Effizienz der aktuellen Versorgungsstrukturen hinterfragen, da der Einsatz von Sozialarbeitenden wesentlich zu einer nachhaltigen Betreuungs- und Begleitungsqualität beisteuern kann. Schlussfolgerung Eine nachhaltige Finanzierung von Sozialarbeitenden in der ambulanten PC trägt zu einer ressourcenschonenderen Betreuung und Begleitung von Sterbenden bei. |
||
|
P64
WIRKLICH WIRKSAMES WISSEN: One Minute Wonder – Schnelles Know-how für Palliative Care!
Michael Rogner, Eschen LI
Abstract
Hintergrund
Das One Minute Wonder (OMW) ist ein evidenzbasiertes Fortbildungsformat aus England, um Wissen in kurzer Zeit zu erweitern. Das OMW fokussiert beispielsweise Themen, wie etwa "Delir" oder die "Surprise Question", auf einer DIN A4-Seite und ist darauf ausgelegt, an Orten wo Wartezeiten entstehen können, gelesen zu werden. Diese effiziente Wissensvermittlung unterstützt die Integration neuer und bestehender Erkenntnisse in die Praxis, ohne dass zusätzliche Ressourcen notwendig sind. Seit 2024 werden OMW in allen Pflegeheimen der LAK eingesetzt, mit einem Fokus auf Palliative Care Know-How. Zu jedem OMW wurde zudem ein begleitendes Video für die interne Wissensplattform erstellt. Ziel
Ziel war es nach der Entwicklung die Akzeptanz und den Nutzen des OMW sowie deren begleitende Videos zu evaluieren. Methode
Dazu wurde eine anonyme Online-Befragung unter 225 Pflegepersonen durchgeführt. Die Befragung erfasste die Lesbarkeit, den Nutzen und die Relevanz der OMW und Videos für die Praxis sowie deren Einfluss auf berufliche Reflexion und den Wissensaustausch im Team. Resultate Auszüge:
Schlussfolgerung Das One Minute Wonder (OMW) hat sich als effektives Fortbildungsformat in den Pflegeheimen der LAK etabliert, das WIRKLICH WIRKSAMES WISSEN in kurzer Zeit vermittelt. Die Ergebnisse zeigen, dass OMW und die begleitenden Videos die Pflegequalität und das berufliche Wissen erweitern und im Bereich der Palliative Care positiv wirken können. |
||
|
P65
Etude qualitative sur les effets de la musicothérapie sur le bien-être de patients hospitalisés en soins palliatifs
Patricia Roh Failletaz, Cully CH
AbstractIntroduction Plusieurs recherches confirment que la musicothérapie (MT) diminue l’anxiété, la douleur et améliore la qualité de vie des patients hospitalisés en soins palliatifs. Elle permettrait au patient de relâcher ses tensions corporelles et psychiques lorsqu’il constate avec impuissance et l’impact de sa maladie incurable sur sa santé, voire l’approche de la fin de sa vie. Grâce à la MT, le patient peut mettre à distance, l’espace d’un instant, sa souffrance et ses douleurs, grâce aux sons d’instruments soigneusement choisis. Au travers de cette étude clinique, nous avons souhaité voir l’impact de la MT sur le bien-être des patients hospitalisés dans notre unité de soins palliatifs. Méthode En raison de la variabilité de l’état physique et psychique des patients en soins palliatifs, mesurer les effets de la MT sur le bien-être des patients rencontre d’importantes difficultés éthiques et méthodologiques et c’est la raison pour laquelle, notre recherche s’est concentrée sur un nombre restreint de patients dans un temps court. Nous avons évalué sur une durée d’une semaine l’effet de 10 séances de MT chez 7 patients âgés entre 52 et 91 ans. La sélection des patients a été faite sur la base de deux critères essentiels : leur accord à recevoir une séance de MT et leur disposition physique et psychique ; les patients trop algiques, asthéniques ou altérés cognitivement étant exclus. L’état général du patient a été mesuré grâce à l’ESAS et d’un questionnaire adapté mesurant le bien-être et l’estime de soi avant et après les séances de MT. Les instruments utilisés ont été : la lyre de rêve, une harpe, un tambour irlandais, deux bols chantants, un balafon, des recueils de chants et des musiques enregistrées en lien avec les affinités du patient. Durant les séances, le patient pouvait se montrer soit actif (par l’emploi d’instruments et/ou de sa voix), soit réceptif (par l’écoute) ou avoir une attitude mixte des deux ; le choix des instruments était libre. Certains patients ont pu bénéficier de plusieurs séances.
Résultats Nos résultats ont montré que les bienfaits des séances de MT ont été décrits en termes de plaisir, de joie, d’oubli de la maladie, de lâcher prise et une diminution de l’anxiété et des douleurs. Certains patients ont diminué leur score de mal être à l’ESAS. Les patients âgés qui avaient tendance à retenir leurs émotions, par peur d’être jugées ou rejetées, ont pu exprimer leurs affects lors des séances de MT ; notamment lorsqu’ils ont « osé » chanter. Les musiques et les chants évocateurs de souvenirs passés, ou renouant avec la culture des patients, étaient les meilleurs supports de travail, et l’attitude réceptive était la préférée des patients. Nous avons également constaté que les patients qui ont pu bénéficier de plusieurs séances ont amélioré leur bien-être ; certains proches nous ont fait remarquer que le patient s’était montré plus ouvert, détendu et apaisé après leur séance de MT. Conclusion Comme plusieurs études l’ont confirmé, la MT a permis à nos patients de se sentir moins anxieux, plus détendus physiquement et psychiquement. Certains nous ont relaté que la MT avait diminué, du moins temporairement, leurs douleurs et amélioré leur humeur et leur sommeil. D’autres ont évoqué un sentiment de meilleure estime de soi, de sécurité, d’apaisement, de tranquillité et « le plaisir d’avoir créé de la musique ensemble ». Dans sa relation avec ses proches, la MT aiderait également le patient à sortir de sa bulle et à se rapprocher des autres. Cette approche thérapeutique s’avère donc un outil essentiel à utiliser auprès des patients hospitalisés en soins palliatifs, mais qui doit être impérativement adapté de cas en cas et pour autant que le thérapeute laisse suffisamment de temps et d’espace à la créativité. Une étude conduite sur une plus longue période et enrôlant un plus grand nombre de patients, voire leurs proches, se justifie au vu des bénéfices observés dans cette étude pilote. |
||
|
P66
Gesundheitliche Vorausplanung (GVP): Erfahrungen von Pflegenden der Onkologie im klinischen Alltag
Céline Rossier, Bern CH
Abstract
Hintergrund
Die gesundheitliche Vorausplanung (GVP) ist bedeutsam in der Betreuung von Patient:innen mit fortgeschrittenen Krebserkrankung, da sie Lebensqualität fördert, Symptome lindert, Stress und Notfalleinweisungen reduziert sowie Angehörige entlastet. Das Bundesamt für Gesundheit sowie die Schweizerische Akademie der Medizinischen Wissenschaften betonen die Relevanz der GVP und fordern deren Verankerung im Gesundheitswesen. Eine routinemässige Umsetzung im klinischen Alltag setzt ein Verständnis der GVP in der Praxis voraus. Dabei kommt Pflegenden eine zentrale Rolle zu. Ziel Die vorliegende laufende Studie ist Teil eines über 4 Jahre angelegten Qualitätsförderungsprojektes zur Umsetzung der «Concurrent Care» das darauf abzielt, GVP parallel zur onkologischen Behandlung zu implementieren. In diesem Teil soll untersucht werden, wie Pflegende die GVP bei Patient:innen mit fortgeschrittenem Krebs wahrnehmen und deren Umsetzung im klinischen Alltag erleben. Im Fokus stehen dabei der Wissensstand der Pflegefachpersonen zu GVP, ihre Erfahrungen sowie wahrgenommene förderliche bzw. hinderliche Faktoren bei der Implementierung von GVP als standardisiertem Prozess im Behandlungspfad. Methode Im Rahmen eines qualitativ - explorativen Forschungsdesigns werden leitfadengestützte Einzelinterviews mit Pflegenden durchgeführt, die im stationären und ambulanten Setting eines onkologischen Zentrums tätig sind. Die Datenanalyse erfolgt der qualitativen Inhaltsanalyse nach. Resultate Bisher wurden sechs der 15 geplanten Interviews mit Pflegenden durchgeführt. Vorläufige Analysen zeigen, dass es für Pflegende herausfordernd war, zu beschreiben, was eine gesundheitliche Vorausplanung ist. In ihrer täglichen Praxis nehmen sie wahr, dass Patient:innen nicht oder zu spät über die Möglichkeiten der Palliative Care informiert werden. Aus Sicht der Pflegenden besteht ein Wissensbedarf und das Anliegen, gesundheitliche Vorausplanung standardisiert in die Versorgung zu integrieren. Schlussfolgerung Die Analyse der Interviews wird bis Oktober 2025 abgeschlossen. Die Ergebnisse sollen aufzeigen, wie die GVP in der onkologischen Behandlung aus der Sicht der Pflegenden derzeit wahrgenommen und umgesetzt wird. Dabei werden sowohl bestehende Wissenslücken als auch praktische Herausforderungen im klinischen Alltag deutlich. An Hand der Ergebnisse werden interprofessionelle Schulungsequenzen angeboten sowie Prozesse überprüft und gegebenenfalls angepasst, damit eine Grundlage für die Umsetzung der GVP im klinischen Alltag entsteht. |
||
|
P67
Physicians’ roles in advance care planning discussions with proxies in long-term care facilities
Eve Rubli Truchard, Lausanne CH
Abstract
Contexte
Advance care planning (ACP) promotes care coherent with patient wishes. ACP participation requires medical decision-making capacity (DMC). ACP participation rates are generally low, and many people lose DMC before formally expressing their wishes for future care. Furthermore, changes in medical situations and unpredictable emergencies make alternative models of ACP necessary for people who have lost medical DMC. We have developed a model specifically for the long-term care context, called ACP by proxy. Information is needed about the ways in which these discussions take place. Here, we examine the roles of physicians in ACP discussions with health care proxies of people who no longer have medical DMC. Objectiv To examine the roles of physicians in ACP discussions with health care proxies of people who no longer have medical DMC. Méthode ACP by proxy discussion for 15 residents in Long Term Care Facilities (LTCF) were audio-recorded during a single-arm pilot intervention study and transcribed verbatim. Discourse analysis was conducted to examine the roles of physicians in these discussions. Résultats Physicians’ roles included providing information about the residents’ current health status, predicting future health conditions, describing illness trajectories and functional capacities, providing information about emergency treatment procedures, risks and benefits, giving advice about reasonable care that is in residents’ best interests, and discussing end-of-life care. Involving healthcare proxies and LTCF professionals in these decision-making processes is a key element of these discussions. Conclusion LTCF physicians play an integral role in ACP for people lacking DMC and draw upon their proximity to LTCF residents and their partnerships with other professional caregivers in order to promote informed anticipatory decision making on behalf of people who have lost DMC. |
||
|
P68
Advance Care Planning by proxy in nursing homes: roles of health professional facilitators
Samira Ruedin, Lausanne CH
AbstractContexte Advance Care Planning (ACP) is effective in promoting care that is coherent with patient wishes and values. ACP requires patients to maintain decision making capacity (DMC). Several calls have been made for advance care planning models for people with dementia, and for people who have lost DMC (ACP- by proxy, ACP-bp). The ways in which these models work, and the roles of the people involved, are yet to be explored. Here, we examine the role of residential aged care health professional (RACF) ACP-bp facilitators in these discussions. Objectiv We aim to examine the role of residential aged care health professional (RACF) ACP-bp facilitators in these discussions. Méthode Semi-structured interviews with RACF health professional, ACP-bp facilitators (n=15), are combined with audio-recorded ACPbp discussions collected as a part of a single-arm pilot intervention study. Thematic analyses were conducted to identify recurring and relevant themes, and these were triangulated post-hoc. Résultats Healthcare professionals described their role as facilitators in ACP-bp as providing counselling, support and mediation. In the ACP-bp discussions, the facilitators draw on their medical knowledge, experience working with people at end of life and without DMC, their proximity to RACF residents, and their liaising role between physicians and health care proxies to guide discussions and co-create treatment plans for future medical emergency. Conclusion RACF health professionals provide a unique and highly valuable skill set and a privileged knowledge of RACF residents, their families and treating physicians which places them well to conduct ACP-bp in RACFs. Furthermore, when provided with the necessary resources and conditions, they can be champions for ACP-bp and are an integral part of ACP-bp implementation. |
||
|
P69
Palliative Care and Heart Failure: Building National Collaboration Between Medical Societities
Piotr Sobanski, Schwyz, Gdansk (Poland) CH
Abstract
Hintergrund
Heart failure (HF) causes high symptom burden and shortens life expectancy. Implementation of Palliative Care (PC) concurrently with cardiologic guidelines-directed medical therapy improves quality-of-life (QoL) more than disease-oriented management alone but is underused. Ziel The Swiss Society of Cardiology (SSC) and the Swiss Society for Palliative Care (palliative.ch) has called the Joint Task Force to implement PC in the comprehesive cardiologic care. Methode Dyads representing cardiology and PC from most Swiss HF centers have accepted the inviation to contribute. Through online voting, workshops, and Delphi process priority topics for the incorporation of PC into standard care for people living with HF have been identified. Resultate 18 experts from 8 Swiss HF centers identified 4 main topics relevant for facilitation of the implementation of PC in the usual care: the timely recognition of the unaddressed health-related needs of affected people and their relatives (by using validated assessment tools), identifying key palliative interventions for the care for people living with HF, identifying strategies to facilitate cooperation between specialist PC and cardiology, defining research agenda to examine the efficacy of PC interventions, quality of care criteria, and outcomes of PC provision in Switzerland. Schlussfolgerung PC helps to alleviate symptoms, psychological distress, existential concerns, and social isolation in people living HF and their relatives. When used concurrently with cardiological care, PC contributes to improved QoL and greater satisfaction with care throughout entire course of living with HF. In the terminal phase, when cardiological management can no longer be optimised or offers minimal benefit, PC continues to provide meaningful support. Achieving benefits depends on the timely recognition of PC needs, the delivery of high-quality, tailored interventions, and the close cooperation between professionals working in cardiology and PC. Overcoming common misconceptions about PC and fostering the ability to early identify unmet needs are essential first steps. Regular assessments of undressed health-related needs throughout the whole trajectory of living with HF, prevents either avoiding inclusion of PC or causing unacceptable delays in integrating PC. Some national societies and regulatory bodies now recommend the introducing PC as early as the home of HF diagnosis. In alignment with these recommendations, the SSC and the palliative.ch advocate for the regular assessment of unaddressed needs - at least when specific triggers evolve - using validated tools: ID-PALL and NAT\:PD-CH. Recognising unmet needs should prompt the evaluation of incorporation a palliative approach into management strategy, but not immediate referral to hospice or PC units. Relying solely on prognosis or risk of death when considering PC is key obstacle that can lead to inadequate care. HF shortens life expectancy and thus necessitates through in-depth communication, which in addition to conveying hope for improvement, should encompass treatment burden, potential failure and the possibility of decline or death - when appropriate and wished. Communication about disease progression is a core competence of PC and can serve as a gateway to collaborative between cardiology and PC professionals. Such communication supports person-centered medical decision making and anticipatory care planing. This statement from the Working Group promotes collaboration between cardiologists, general practitioners, PC professionals, and others by identifying existing barriers and proposing strategies to overcome them. Further steps in advancing the field of comprehensive care for people living with HF include evaluating the effectiveness of approach, cost-effectiveness and establishing a future research agenda |
||
|
P70
Comparaison des réseaux de soins palliatifs suisse et kirghize dans la prise charge d'une douleur
Simon Singovski, Collonge-Bellerive CH
Abstract
Contexte
Depuis une vingtaine d'années s'est instaurée une coopération en matière de soins palliatifs entre la Suisse et le Kirghizistan. Entre 2007-2024 dans le cadre du projet « Medical Education Reform (MER) » de la Direction suisse du Développement et de la Coopération (DDC) et des Hôpitaux Universitaires de Genève (HUG), par la suite avec le soutien de la Fondation F. et J. Maurice "la médecine au service du développement". Cette coopération a été active dans la formation et le soutien de médecins palliativistes, pionniers au Kirghizistan, et les a accompagnés face aux nombreux défis posés par le développement des soins palliatifs dans un pays aux ressources limitées. Objectiv L'objectif primaire est d'analyser les points communs et les différences entre les réseaux de soins palliatifs suisses et kirghizes. L'objectif secondaire est de mettre en avant les progrès atteints grâce à la coopération Suisse-Kirghizistan, et d'identifier les axes de développement futurs. Méthode Echange entre plusieurs spécialistes en soins palliatifs des deux pays (2 médecins et 1 infirmière suisses, 2 médecins kirghizes) afin d'identifier les ressources, le réseau et les obstacles existants lors de la prise en charge d'une urgence palliative à domicile dans le cadre d'une crise douloureuse nociceptive sévère. Résultats Plusieurs différences notables entravent un soulagement rapide des douleurs au Kirghizistan, comparé à la Suisse : manque de personnel formé et de structures spécialisées dans les soins palliatifs, indisponibilité de la morphine et ses dérivés, opiophobie des médecins de ville, des patients et des familles, obstacles techniques et administratifs à la prescription de la morphine. Le financement est garanti en Suisse par l'assurance obligatoire, alors qu'il est insuffisant et incomplet au Kirghizistan. Discussion Les interventions de notre délégation auprès du réseau kirghize de soins palliatifs ont permis de renforcer le développement des soins palliatifs dans ce pays. Elles ont amené à des changements législatifs et administratifs, davantage d'accès à la morphine, une meilleure reconnaissance des soins palliatifs par les facultés de médecine ainsi qu'à une meilleure information des médecins, des soignants de premier recours et des pharmaciens. Conclusion Il existe plusieurs barrières à l'accès aux soins palliatifs et aux opiacés au Kirghizistan, dont une partie a pu être partiellement levée à travers la collaboration Suisse-Kirghizistan. La comparaison entre les deux pays permet d'apprécier les acquis obtenus en Suisse depuis les années 80', mais également de définir certains objectifs importants pour le développement des soins palliatifs au Kirghizistan. |
||
|
P71
Palliativement inclusif
Chiara Soloni, Locarno CH
Abstract
Contexte
La disabilità intellettiva colpisce circa l'1-2% della popolazione mondiale. Le persone con disabilità intellettiva vivono forti disuguaglianze di salute e di presa in carico palliativa. Comprendere le cause di queste disuguaglianze è importante per poter lavorare allo sviluppo di una cultura per l’attivazione precoce di un approccio palliativo, soprattutto per le persone con disabilità cognitiva istituzionalizzate. Concretizzare una strategia coordinata che risponda puntualmente al crescere dei bisogni palliativi delle persone con disabilità cognitiva che invecchia (come tutta la popolazione) nelle strutture sociosanitarie: diventa una urgenza socioassistenziale.
Objectiv La scarsità di interventi specialisti di cure palliative (CP), il crescere dei bisogni in una popolazione specifica che invecchia con esigenze speciali richiedono una risposta puntuale nella fornitura di CP. È urgente sviluppare un modello di partnership flessibile e cooperativa tra fornitori di CP generale e specialistico incorporando la formazione la collaborazione ed il dialogo tra CP all’interno delle strutture dove le persone con disabilità risiedono o vivono e tutto il personale socio/educativo-sanitario-assistenziale. È richiesta dialettica reciprocità e formazione continua. La formazione è il modo migliore per implementare l'assistenza e la presa in carico palliativa precoce. Come ci chiedono gli Utenti: “Noi vogliamo sapere cosa ci sta succedendo perché... Abbiamo delle scelte da fare... “ Méthode Le persone con disabilità cognitiva dalla nascita hanno vissuto e continuano a vivere varie forme di pregiudizio, privazione dei diritti civili e accesso alle cure, comprese anche, quelle palliative. Proponiamo un modello di offerta di CP che cerchi di incorporare la realtà della vita quotidiana della disabilità con un confronto continuo specialistico palliativo al fine di offrire una presa in carico congiunta, anticipatoria e ricercando il coinvolgimento della persona disabile e delle sue volontà. Il progetto, nato in un singolo istituto, mira a creare un gruppo interdisciplinare di collaborazione composto da personale socioeducativo-assistenziale-sanitario - professionisti formati dedicati alla cura quotidiana (CP generali) - che si confronta sistematicamente con professionisti di CP specialistiche consulenti per individuare e monitorare bisogni speciali palliativi delle persone con disabilità cognitiva nella loro evoluzione. Un primo step è rappresentato dalla formazione/sensibilizzazione alle CP di tutto il personale socioeducativo-assistenziale (educatori, operatori, ergoterapisti, fisioterapisti logopedisti, infermieri …) e i medici attivi nelle strutture dove vivono le persone. Approfondire la conoscenza riduce le paure sulle capacità di comprensione verso l'informazione e permette il coinvolgimento nell'assistenza diretta. Grazie alla condivisione dell’esperienza e il lavoro interattivo e reciproco tra le diverse parti, l’intervento potrà essere migliorato. Il personale educativo-assistenziale della struttura - sensibilizzato e formato - identifica i bisogni di CP dei residenti in modo oggettivo, si confronta con il personale sanitario della struttura ed in base ai bisogni (palliative generali o specialistiche) viene attivato il team di consulenza specialistica palliativa. Il team analizza i bisogni e redige un piano di presa in carico condiviso. Progetto di presa in carico condiviso in cui le persone con disabilità cognitiva e le loro famiglie vengono coinvolte – secondo il loro grado di comprensione e comunicazione – nei processi decisionali riguardanti il loro stato di salute dal team specialistico palliativo che interviene in consulenza in struttura. Résultats
Conclusion Per migliorare la qualità dell’offerta sanitaria alle persone con disabilità è necessario sviluppare un servizio di collaborazione tra un approccio generale socio-educativo-assistenziale ed un approccio specialistico palliativo: il lavoro insieme e l’apprendimento congiunto tra personale che opera all’interno di istituti per persone con disabilità e CP specialistiche sono vissuti come fondamenti di crescita reciproca. Sono necessarie collaborazioni e soprattutto formazione di CP agli operatori socio-educativo-assistenziali dei servizi per persone con disabilità cognitiva deve cresce la conoscenza reciproca ed il sapere intorno a queste persone che vivono la normalità nella loro diversità. È importante sensibilizzare e formare anche il “mondo medico” per implementare la collaborazione ed il confronto palliativo intorno alla persona con disabilità cercando di superare le paure ed i pregiudizi. I professionisti specialisti di CP hanno il dovere di chinarsi alla conoscenza di queste specificità di vita per rispondere a bisogni sempre più crescenti di questa popolazione che invecchia e che richiede quindi, una presa in carico specifica. Gli operatori socio-educativo-assistenziali hanno la responsabilità di “tradurre” il sapere di queste persone affinché gli specialisti che intervengano possano capire il mondo delle persone con disabilità ed offrire loro una cura adeguata e personalizzata. È importante riconoscere che la formazione e l'istruzione da sole non funzioneranno è urgente la necessità di sostenere lo sviluppo di sistemi di collaborazione tra saperi. Questi sistemi devono creare nella collaborazione, ambienti di cura adeguati in cui i professionisti siano facilitati nel lavoro multidisciplinare e in una maggiore collaborazione e dialogo tra professionisti, pazienti e i loro amici/familiari. Come ci insegna un nostro Utente: “Noi abbiamo bisogno di tranquillità affetto e di solidarietà… Mi piace parlare con voi perché mi ascoltate sempre” Solo nella collaborazione e nella reciprocità della condivisione dei saperi si può vivere un approccio “palliativamente inclusivo” aperto alla vita ed al rispetto delle scelte di vita delle persone con disabilità cognitiva. |
||
|
P72
Gesundheitslots:innen als ethisch koordinierende Vertrauenspersonen in komplexen Versorgungssituationen
Jürg Streuli, Zürich CH
Abstract
Hintergrund
Menschen mit komplexen chronischen Erkrankungen stehen oft vor einer unübersichtlichen Versorgungslandschaft mit fragmentierten Zuständigkeiten, unklarer Kommunikation und einem hohen emotionalen Belastungsniveau. In solchen Situationen braucht es nicht nur medizinische, sondern auch ethische Orientierung und Vertrauenspersonen, die die verschiedenen Perspektiven auf "gute" Entscheidungen aufzeigen, moderieren und ggf. abwägen helfen. Ziel Die Gesundheitslots:innen bieten basierend auf einem zeitlich befristeten Auftrag (optimalerweise während 3 Monate) ein intensives ethisches Case Management, mit Verknüpfung und Koordination bestehender Ressourcen, Organisation und Moderationen interprofessioneller Gespräche und Begleitung von Entscheidungen mit hoher Eingriffstiefe entlang bio-psycho-sozio-spiritueller Leitziele mit Hilfe von strukturierten Rundtischen, ethischen Gesprächen und persönlicher Begleitung. Methode Im Rahmen eines partizipativen Entwicklungsprojekts wurden Gesundheitslots:innen als neue Rolle im Schweizer Versorgungssystem konzipiert. Sie begleiten Patient:innen und ihre Familien kontinuierlich über institutionelle, professionelle und sektorale Grenzen hinweg. Dabei kombinieren sie Elemente von Shared Decision-Making, Ethikberatung, Koordinationsarbeit und psychosozialer Begleitung. Die Lots:innen werden interprofessionell geschult – mit einem besonderen Fokus auf ethische Reflexionskompetenz, kultursensible Kommunikation und Strukturierung von Entscheidungsprozessen. Resultate Die Rolle der Gesundheitslots:in wurde entlang folgender Dimensionen definiert um die vorhandenen Ressourcen und Angebote zu identiziferen, zu verbinden und zu koordinieren:
Diskussion Die Rolle der Gesundheitslots:innen eröffnet neue Perspektiven, Chancen und Zugänge für eine integrierte, wertebasierte Versorgung insbesondere in palliativen, chronischen und vulnerablen Kontexten. In einer nächsten Projektphase werden Schulungsprogramme implementiert und erste Erfahrungen aus der Praxis systematisch evaluiert. Schlussfolgerung Die bisherigen Erfahrungen und das vorgestellte Konzept verdeutlichen das Potenzial von Gesundheitslots:innen, die Versorgungsqualität und -kontinuität spürbar zu verbessern. Sie stärken die ethische Resilienz aller Beteiligten, fördern Entscheidungsklarheit und erleichtern durch ihre koordinierende Rolle den rechtzeitigen und angemessenen Zugang zu Palliative Care – insbesondere durch eine gezielte Aufgabenverteilung im transprofessionellen Netzwerk. |
||
|
P73
Vorausschauende Behandlungsplanung bei hochaltrigen Menschen mit Frailty – eine Einzelfallanalyse
Simone Suter, Winterthur CH
Abstract
Hintergrund
Die frühzeitige Kommunikation von Behandlungspräferenzen im Rahmen der vorausschauenden Behandlungsplanung (Advance Care Planning, ACP) ist für alle Personen relevant. Bei älteren Menschen mit Frailty-Syndrom (Gebrechlichkeit) werden diese Gespräche in der Praxis trotz hoher Relevanz allerdings noch immer selten umgesetzt.
Ziel Die Identifikation des geeigneten Zeitpunkts für ein vorausschauendes Gespräch stellt im pflegerischen Alltag eine Herausforderung dar. Methode Im Rahmen einer Fallbeschreibung mit anschließender systematisierter Literaturrecherche setzten sich Studierende des Bachelorstudiengangs Pflege mit dieser Thematik auseinander und identifizierten relevante Schlüsselmomente für ihr zukünftiges berufliches Handeln. Resultate Fallbeschreibung: Schlussfolgerung Konklusion: |
||
|
P75
Soins palliatifs et essais cliniques en oncologie : un (in)dissociable duo ? Scoping review
Martyna Tomczyk, Lausanne CH
Abstract
Contexte
Les essais cliniques visant à tester une nouvelle option thérapeutique antitumorale constituent un pilier primordial de la recherche en oncologie. Si l’intégration des soins palliatifs à ces investigations est techniquement faisable et recommandée, elle n’est pas systématique ; les soins palliatifs sont généralement considérés comme une alternative à un essai clinique, et non comme partie intégrante. À ce jour, les facteurs favorisant ou empêchant l’intégration des soins palliatifs en complément d’un essai clinique sont très peu explorés. Objectiv L’objectif de notre étude est de mieux comprendre les facteurs qui favorisent ou empêchent l’intégration des soins palliatifs aux essais cliniques chez les patients adultes atteints d’un cancer solide ou hématologique, toutes situations cliniques et toutes phases d’essai confondues. Méthode Afin d’atteindre notre objectif, nous avons choisi de réaliser une scoping review. Résultats Des stratégies de recherche ont permis d’identifier 2262 textes, dans la base de données Embase.com, sans restriction d’année de publication. À ce jour – au 30 mai 2025 –, nous sommes dans le processus de sélection manuelle des textes appropriés en fonction de leurs titres et de leurs résumés, et conformément à nos critères d’inclusion. Ainsi, sont progressivement considérés pour inclusion tous les types de textes pertinents en anglais (études empiriques, revues systématiques, textes réflexifs, consensus d’experts, résumés de présentation en congrès, cas cliniques, etc.), excepté les protocoles de recherche. Les textes ainsi inclus seront étudiés à partir d’une grille d’analyse préalablement élaborée. Conclusion L’identification des facteurs favorisant et empêchant l’intégration des soins palliatifs en complément d’un essai clinique permettra de mieux cerner cette situation complexe, d’en saisir les nuances et de proposer des pistes de réflexion en vue des actions concrètes au bénéfice des personnes malades. La présentation des résultats issus de cette étude internationale au public suisse, lors du congrès de Bienne, nous donnera l’opportunité d’en discuter les enjeux pour la Suisse. |
||
|
P76
Psychothérapie assistée par la Kétamine(PAK): une approche de la détresse en soins palliatifs ?
Anne Vacanti-Robert, Blonay CH
Abstract
Contexte
Objectiv Présentation de la PAK Méthode Etude de cas: Mme X, 66 ans, est atteinte d’un cancer du sein métastatique osseux depuis 2021. Elle présente un état anxio-dépressif chronique, une fatigue accablante et des ruminations anxieuses autour de la mort. Elle exprime un sentiment d’impasse, associé à une détresse existentielle majeure, et évoque la possibilité d’un suicide médicalement assisté. Malgré un suivi psychothérapeutique intensifié et une adaptation des traitements antidépresseurs, aucune amélioration n’est observée. Dans ce contexte, une psychothérapie assistée par la kétamine lui est proposée, encadrée par un médecin palliativiste et un psychiatre formés à cette approche. Résultats Après deux séances préparatoires, une administration de kétamine sublinguale (120 mg) est réalisée en ambulatoire, en présence des thérapeutes. Une amélioration notable de l’humeur, de la fatigue et de l’énergie est observée dès la première semaine. L’intégration post-séance, facilitée par l’expression artistique, permet de travailler les prises de conscience issues de l’expérience. Une seconde séance a lieu trois mois plus tard, au cours de laquelle la patiente vit une expérience mystique intense, marquée par un sentiment d’unité et d’amour persistant plusieurs semaines. Elle décrit une meilleure acceptation de sa situation et un apaisement de la peur de mourir. Conclusion Ce cas illustre le potentiel transformateur de la PAK dans la prise en charge de la détresse existentielle en soins palliatifs. Les dessins de la patiente en témoignent. En mobilisant les états modifiés de conscience dans un cadre psychothérapeutique structuré, la PAK pourrait offrir un espace de réconciliation là où les approches conventionnelles montrent leurs limites. Elle s’impose ainsi comme une approche complémentaire prometteuse, contribuant à restaurer du sens, à améliorer la qualité de vie et à accompagner la fin de vie avec plus de sérénité. 

|
||
|
P77
Implementierung von patientenzentrierten Messinstrumenten in der häuslichen Palliativversorgung
Ankie van Es, Zürich CH
Abstract
Hintergrund
Gemäss nationalen und internationalen Qualitätsstandards sollen patientenzentrierte Ergebnismessinstrumente (PROMs) routinemässig in der spezialisierten Palliative Care eingesetzt werden. Ziel Wir haben in der Spitex Palliaviva die nachhaltige Einführung der PROMs untersucht. Methode Die Implementierung der PROMs orientierte sich am Consolidated Framework for Implementation Research (CFIR). Nach einer initialen Schulung wurden die PROMs (Australischer Karnofsky Performance Status (AKPS), Integrated Palliative Care Outcome Scale (IPOS) und Palliativphase) systematisch bei allen Patient:innen eingesetzt. Die Palliativphase, AKPS, und IPOS wurden bei jedem Besuch / Telefonat eingeschätzt und im elektronischen Dokumentationssystem anhand einer adaptierten Übersichtsdarstellung festgehalten. Die Implementation wurde intern von einem klinischen Champion und punktuell während Teamsitzungen auch von einem Quality Improvement Facilitator begleitet. Resultate Seit der Einführung der PROMs vor 15 Monaten werden bei sämtlichen Patient:innen systematisch die PROMs eingesetzt. In regelmässig stattfindenden Teamsitzungen wird der Einsatz der PROMs in der Praxis reflektiert. Die Integration der IPOS-Struktur in das SENS-Modell bei Eintrittsdokumenten, die Etablierung einer einheitlichen Darstellung der PROMs-Daten sowie die kontinuierliche Nutzung von IPOS, AKPS und der Palliativphase im Austrittsbericht führten zu mehreren, zunächst nicht antizipierten Effekten. Dazu zählten (a) eine konsequentere Priorisierung vom Handlungsbedarf aus Sicht der Patient:innen sowie (b) eine effizientere und strukturierte Informationsweitergabe an beteiligte Leistungserbringende im Gesundheitswesen. Im Hinblick auf den internen Nutzen der PROMs-Daten für qualitätsbezogene Verbesserungsprozesse wurden bestehende Vorbehalte thematisiert und Präferenzen hinsichtlich zukünftiger Datenauswertungen, insbesondere bezüglich der Visualisierung von Wirksamkeit, identifiziert. Schlussfolgerung Die Implementierung von PROMs wird von Pflegenden im klinischen Alltag zunächst als zusätzlicher Aufwand wahrgenommen. Die vorliegenden Ergebnisse zeigen, dass durch eine strukturierte Integration in bestehende Dokumentations- und Kommunikationsprozesse sowie durch regelmäßige Reflexion für das Team ein Mehrwert entsteht. Eine offene Kommunikationskultur während des Implementierungsprozesses erwies sich dabei als zentral für die nachhaltige Verankerung der PROMs in der spitalexternen Palliative care. |
||
|
P78
Soins palliatifs au domicile des patients atteints de SLA : retour d’expérience
Petra Vayne-Bossert, Genève CH
Abstract
Contexte
Les soins palliatifs améliorent la qualité de vie des personnes atteintes de maladies évolutives, notamment neurologiques. La sclérose latérale amyotrophique (SLA), caractérisée par un affaiblissement musculaire progressif, s’accompagne de symptômes physiques (douleurs, dyspnée) et psychiques (angoisse, dépression), nécessitant une prise en charge globale et précoce. Aux Hôpitaux Universitaires de Genève (HUG), une collaboration entre le Centre pour la Sclérose Latérale Amyotrophique (CeSLA) et l’équipe de soins palliatifs à domicile (CoSPa dom) permet d’assurer ce suivi, notamment pour les patients ne pouvant plus se déplacer chez leur médecin. Objectiv Analyse de la pratique actuelle après 17 mois de mise en place pour permettre une évolution et une amélioration de la prise en charge de ces patients et notamment la coordination entre deux services différents. Méthode Cette évaluation porte sur les interventions de la CoSPa dom depuis janvier 2024. Analyse du nombre de patients SLA suivi au domicile ; la durée du suivi et le nombre de consultation ; contexte de référence de ces patients ; souhait et lieu du décès de ces patients ; symptômes des patients et de leurs gestions. Echange avec le groupe CeSLA autour de ces résultats pour améliorer nos pratiques et la prise en soin de ces patients. Résultats En 17 mois, 13 patients atteints de SLA ont été suivis, avec une moyenne de 297 jours d’accompagnement et 68 consultations à domicile. Les patients ont été référés principalement par leur médecin traitant (3), des collègues palliativistes (4) ou suite à une hospitalisation (5), mais rarement par les neurologues (1). Actuellement, 9 patients sont encore suivis, 2 ont été transférés vers un suivi de premier recours, et 2 sont décédés. Un premier échange entre le service de médecine palliative et le CeSLA a conclu à une amélioration de la collaboration notamment en matière de référence des patients vers notre service dès que possible. Des critères spécifiques ont été établis et sont revus régulièrement. Les palliativistes vont désormais participer activement au groupe du CeSLA lors de leurs colloques mensuels. Conclusion La prise en charge palliative à domicile s’avère pertinente dès que les déplacements deviennent difficiles, assurant la continuité des soins en lien avec l’équipe CeSLA. Une meilleure coordination interdisciplinaire au moment de l’orientation vers les soins palliatifs est toutefois nécessaire pour assurer une prise en charge précoce. Une évaluation approfondie de l’impact de ces interventions est en cours. |
||
|
P79
"Nichts über uns ohne uns!" - Auch nicht in der Palliative Care
Corinne Wohlgensinger, St. Gallen CH
Abstract
Hintergrund
Das Recht auf Selbstbestimmung ist in der Palliative Care und der UN-Behindertenrechtskonvention zentral, stellt aber insbesondere am Lebensende Fachpersonen und Institutionen vor ethische Herausforderungen. Das partizipative Team SEGEL („Schwierige Entscheide – Gemeinsame Lösungen“) hat einen Gesprächsleitfaden entwickelt, um schwierige Fragen rund um Selbstbestimmung gemeinsam (Fachleute und Menschen mit Beeinträchtigungen) zu bearbeiten. Ziel Das Team SEGEL untersucht, wie Menschen mit kognitiven Beeinträchtigungen gleichberechtigt an ethischen Entscheidungsprozessen beteiligt werden können. Der gemeinsam entwickelte und spielerisch aufbereite Gesprächsleitfaden und ein entsprechendes Poster werden an der Tagung vorgestellt. Methode
Resultate
Schlussfolgerung Partizipative ethische Entscheidungsfindung ist ein wirksamer Ansatz, um die Rechte und Bedürfnisse von Menschen mit kognitiven Beeinträchtigungen auch in der Palliative Care zu stärken. Die entwickelten Instrumente und Methoden sind auf andere Kontexte übertragbar und leisten einen Beitrag zu mehr Selbstbestimmung, Teilhabe und menschenrechtsbasierter Praxis. |
||
|
P80
Parents’ expectations regarding case management for rare diseases in Switzerland
Ursula von Mengershausen, St. Gallen CH
Abstract
Hintergrund
Rare diseases often involve complex, multisystem conditions, placing a high burden on families—particularly when affected children require multidisciplinary care. Case management (CM) is considered a promising approach to improve care coordination, yet little is known about parental perspectives on CM in this context. Ziel This pilot study aims to enhance understanding by examining parents’ specific views onthe requirements, content and objectives of case management and advanced care coordination for children with rare diseases during childhood. The findings of this study are expected to offer valuable insights and recommendations for existing and future initiatives in clinical practiceand research, with the goal of improving the comprehensive, child-centred and family-orientated approach to case management. Methode An online survey was distributed to members of the Swiss Children with Rare Diseases (KMSK) network. Of 775 invited families, 108 responded (14% response rate). The survey included both structured questions (e.g. Likert scales on quality of life, care needs, and satisfaction) and open-ended responses, which were analysed using Mayring’s qualitative content analysis. Quantitative data were analysed descriptively and via chi-squared tests. Resultate The study included 108 respondent families from among the 775 in the KMSK, a 14% response rate.The age of their children ranged from 0.4 to 24 years (mean: 8) and their level of suffering in the past six months varied, with 31.5% indicating intense or very intense suffering. In terms of case management, 15.8% of families re-ported access while 32.4% expressed a need but did not have access to it. The study identified three categories of parental expectations regarding case management, emphasising the importance of interprofessional collaboration, effective communication and comprehensive support. Diskussion The study highlights a significant gap between the need for and availability of CM among families of children with rare diseases. Parents described CM as a crucial role that extends beyond logistics to include emotional, communicative, and advocacy functions. Findings suggest that CM could relieve systemic burdens and improve family-centred care, but must be tailored to complex realities. Schlussfolgerung The findings shed light on the high need for case management support with a current undersupply in Switzerland and an association with reduced parental quality of life, highlighting the necessity for diverse supportand assistance to effectively manage the challenges facedby families with children with rare diseases. |
||
|
P81
"Enjeux palliatifs" : un serious game pour explorer les soins palliatifs de façon immersive.
Joelle Zuber, La Chaux-de-Fonds CH
Abstract
Contexte
Le travail de soignant en soins palliatifs requiert des compétences cliniques, relationnelles et éthiques spécifiques. Ces thématiques sont peu abordées dans les formations initiales des professionnel.le.s de santé et évoluent selon les expériences des soignant.e.s durant leur parcours professionnel. Objectiv Renforcer l’apprentissage actif par l’expérimentation dans un environnement sécurisé et interactif. Permettre une évaluation formative continue des acquis via des feedbacks intégrés. Méthode « Enjeux palliatifs » est un jeu de plateau pédagogique destiné aux équipes soignantes, centré sur l’acquisition des compétences fondamentales en soins palliatifs. Basé sur une situation clinique réaliste, le jeu plonge les participant.e.s dans le quotidien d’une équipe pluridisciplinaire accompagnant un.e patient.e en phase palliative. Le but du jeu est de maintenir ou améliorer la qualité de vie de la personne soignée à travers des décisions cliniques collectives, des dilemmes éthiques ou des échanges sur les bonnes pratiques. Le jeu aborde notamment la communication avec les patient.e.s ou les proches, l’identification des symptômes et la coordination des interventions. Le format ludique favorise l’engagement, la réflexion en groupe et la dédramatisation de situations souvent vécues comme complexes. Chaque session de jeu dure environ vingt minutes et peut être animée dans un cadre de formation continue ou lors de séminaires interprofessionnels. Résultats Testé auprès d’un groupe pilote d’infirmièr.e.s ce jeu a suscité un fort intérêt et permis une meilleure appropriation des principes de la démarche palliative et des concepts abordés durant la session de formation. Les retours mettent en avant la richesse des échanges suscités, l’ancrage dans la réalité clinique et la capacité du jeu à rendre visible les dynamiques d’équipe.
Conclusion Ce dispositif innovant se veut un outil complémentaire aux approches pédagogiques usuelles, afin de sensibiliser et former des soignants de manière participative et concrète. |
||
|
P82
Caring Community e cure palliative: il modello di Lodi per una rete di cura narrativa e territoriale
DANILA Zuffetti, LODI IT
AbstractContexte La città di Lodi (Lombardia, Italia) presenta un’elevata incidenza di tumori e una significativa popolazione di pazienti cronici. Tale contesto ha evidenziato il bisogno di una rete comunitaria stabile, capace di affrontare fragilità, vulnerabilità, morte e dolore con approcci multidimensionali e intergenerazionali. Da febbraio 2024 è attivo il programma Caring Community di Lodi, volto a sensibilizzare e coinvolgere cittadini, scuole, istituzioni e associazioni, ispirandosi alla Carta delle Città Compassionevoli. Lodi è tra le prime città italiane ad aver strutturato e formalizzato il proprio impegno con la Dichiarazione Lodi Caring Community 2025. Objectiv Diffondere la cultura delle cure palliative a livello territoriale, promuovendo benessere, consapevolezza e risposte concrete. Méthode Il programma ha previsto:
Résultats Nel 2024 la rete contava 8 enti, saliti a 23 nel 2025. Le attività svolte includono: Conclusion Lodi rappresenta un modello integrato e innovativo di Caring Community. Nel 2025 le azioni sono state ampliate, coinvolgendo tutte le fasce d’età e promuovendo una cultura della cura diffusa e concreta, che integra narrazione, relazione e responsabilità collettiva.
|
||
|
P83
NaMPaC Model®: medicina narrativa per la presa in carico in ambiti palliativi e cronici
DANILA Zuffetti, LODI IT
Abstract
Contexte
Le cure palliative, intese nella loro accezione estesa, richiedono approcci innovativi che integrino la dimensione clinica con quella esistenziale e relazionale. In questo quadro nasce il NaMPaC Model® (Narrative Medicine in Palliative Care), il primo modello strutturato e specifico di medicina narrativa per questi contesti. Il modello si distingue dalla semplice raccolta anamnestica o biografica, configurandosi come un percorso continuativo, clinicamente integrato Objectiv Promuovere una presa in carico globale della persona malata, migliorando la qualità della vita di pazienti, familiari e professionist Méthode Dal 2015, il modello è stato applicato in molteplici setting di cura: hospice, assistenza domiciliare, servizi territoriali e reparti oncologici. È prevista la presenza costante di un’esperta in medicina narrativa e cure palliative, integrata all’équipe. Il percorso si articola in fasi, dalla presa in carico iniziale fino al decesso, alla dimissione o alla conclusione del trattamento. Il modello, fondato su basi epistemologiche e operative solide, non si sovrappone agli interventi psicologici o volontari, ma costituisce una pratica clinica autonoma. I feedback narrativi vengono regolarmente restituiti ai professionisti per tradurre i bisogni emergenti in azioni concrete di cura. Résultats L’applicazione del NaMPaC Model® ha favorito l’ottimizzazione del lavoro d’équipe, l’emersione di bisogni latenti, volontà e vissuti del paziente, incrementando la consapevolezza individuale. Dal 2015 sono state raccolte oltre 1.000 narrazioni in ambito palliativo, oncologico, cronico e nelle malattie rare. Conclusion Il NaMPaC Model® è stato presentato e implementato in numerosi contesti nazionali e internazionali. È attualmente l’unico modello strutturato e codificato di medicina narrativa specifico per le cure palliative a livello globale. Dimostra l’efficacia dell’integrazione tra scienze umane e pratica clinica per una presa in carico globale e relazionale della persona.
|